- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
- Web Stories
What Is HKU5-CoV-2? The New Coronavirus Discovered In Bats By Chinese Researchers

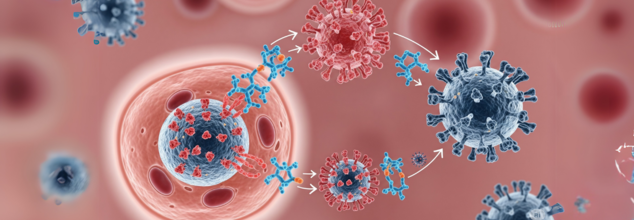
Chinese scientists at the Wuhan Institute of Virology have discovered a new coronavirus strain, HKU5-CoV-2, that is similar to SARS-CoV-2, the COVID-19 virus. The research, released in the journal Cell, has created scientific interest and public interest. Even though HKU5-CoV-2 has not yet been isolated from humans, the fact that it can bind to human receptors calls for more investigation.
What is KHU5-CoV-2?
HKU5-CoV-2 is a member of the subgenus Merbecovirus, which comprises other coronaviruses such as the Middle East respiratory syndrome (MERS) virus. The virus was first found in Pipistrellus bat species in Hong Kong. Recent laboratory tests show that HKU5-CoV-2 possesses the ability to bind to angiotensin-converting enzyme 2 (ACE2) receptors, the same receptors used by SARS-CoV-2 for infecting human cells. This has implications regarding its possible animal-to-human transmission.
Is HKU5-CoV-2 Similar to SARS-CoV-2?
The HKU5-CoV-2 is notable because, like SARS-CoV-2, the viruses utilize the ACE2 receptor to enter the cells of human beings. Even so, the scientists point out that HKU5-CoV-2 efficiently attaches to receptors of human cells far less effectively compared to SARS-CoV-2 and is thus human-to-human transmission highly unlikely. In laboratory testing, HKU5-CoV-2 infection is demonstrated with human lung cells, but they are not found to have that easy transmissibility that infected SARS-CoV-2 into a world pandemic.
The finding has also sparked renewed controversies surrounding the activities of the Wuhan Institute of Virology, the very same research institute blamed for unleashing the COVID-19 virus. Headed by celebrated virologist Dr. Shi Zhengli, dubbed the "bat lady," the research group has been investigating bat coronaviruses for decades to identify potential zoonotic risks. The discovery of HKU5-CoV-2 has sparked new controversy, especially as stock values of some vaccine makers skyrocketed after the announcement.
Can HKU5-CoV-2 Infect Humans?
To date, there is no direct evidence that HKU5-CoV-2 can infect humans. The study recognizes that the possibility of animal-to-human spillover is still unknown. Nevertheless, since coronaviruses have previously jumped species barriers—like SARS, MERS, and COVID-19—scientists are still wary. The World Health Organization (WHO) has pointed out that ongoing surveillance of bat-borne coronaviruses is needed to avoid future outbreaks.
Role of Merbecoviruses in Human Health
HKU5-CoV-2 belongs to the Merbecovirus subgenus, which contains:
MERS-CoV: The Middle East respiratory syndrome virus, with a 36% fatality rate in confirmed cases.
Tylonycteris bat coronavirus HKU4: Isolated from bats but not reported to infect humans.
Hedgehog coronavirus 1: Infects mainly hedgehogs and is not associated with human disease.
The identification of HKU5-CoV-2 contributes to the increasing body of evidence suggesting that Merbecoviruses may be potential threats to human health. Despite the fact that HKU5-CoV-2 has no association with human cases, the fact that it can bind with ACE2 receptors makes it deserving of further studies.
What Does This Mean for Public Health?
Although HKU5-CoV-2 is not found in humans, its emergence highlights the importance of monitoring zoonotic diseases proactively. Global health experts emphasize that:
Track bat populations: Since bats are natural reservoirs of numerous viruses, there must be ongoing monitoring.
Identifying receptor interactions: Studies of the binding of coronaviruses to human receptors can aid in evaluating spillover risks.
Investment in pandemic readiness: The COVID-19 pandemic served to remind us of the importance of early discovery and response measures to new viruses.
Researchers will continue to investigate HKU5-CoV-2 to find out its possible risks. The future research will involve:
- The capacity of the virus to mutate and evolve to suit human hosts.
- Possible animal intermediaries that might be used for transmission.
- Vaccine and therapeutic advancements to counteract emerging coronaviruses.
The identification of HKU5-CoV-2 serves as a reminder that coronaviruses are still a public health issue worldwide. Although there is no immediate human threat, the discovery emphasizes the need for caution in monitoring and investigating zoonotic infections. Ongoing research and surveillance are essential in avoiding future pandemics and preparing the world for emerging viral threats.
Efficient mRNA May Reverse And Rid The Body Of HIV- New ‘Medical Miracle’ Treatment Sparks Global Buzz
Credits: Health and me
In a breakthrough widely hailed as a potential game-changer in the battle against HIV, scientists at Australia's Peter Doherty Institute for Infection and Immunity have made a discovery for a new method to expose the virus that lurks inside human cells. The innovative mRNA-based technology has the potential to lead the way to the long-desired cure for HIV—a condition that has infected millions worldwide and remains uncurable in spite of years of advances in medicine.
One of the biggest challenges to curing HIV is the virus's capacity to "hide" within some white blood cells. These viral reservoirs, which remain hidden, enable HIV to escape immune and antiretroviral detection. Despite medication possibly bringing the virus down to undetectable levels in the blood, latent HIV may persist within these cells and re-emerge, making patients a constant risk and requiring a lifetime of treatment.
Conventional therapies are able to suppress HIV replication but not eradicate these reservoirs. A cure has therefore been elusive—until now.
The mRNA Breakthrough
Building on the promise of mRNA technology, which made headlines worldwide during the COVID-19 pandemic, researchers at the Doherty Institute developed a targeted delivery system based on lipid nanoparticles (LNPs) to deliver mRNA directly to HIV-infected white blood cells.
Injecting mRNA into these cells was previously impossible since these white blood cells do not easily take up the lipid nanoparticles commonly employed for mRNA delivery. The researchers overcame this obstacle by designing a new lipid nanoparticle—designed as LNP X—and these enigmatic cells readily take it up.
Once inside the cell, the mRNA tells the cells to make signals that effectively "unmask" the virus, rendering the concealed HIV detectable by the immune system and medicines.
Dr. Paula Cevaal, a research fellow at the Doherty Institute and co-first author of the landmark study published in Nature Communications, described the team’s reaction to their initial findings as one of disbelief and excitement. “We were overwhelmed by how much of a night and day difference it was—from not working before, and then all of a sudden it was working. All of us were just sitting gasping like, ‘wow’,” she told The Guardian.
The findings have been reproduced repeatedly in the laboratory with blood cells from HIV-infected donors. Although the research is still at the cellular level, the discovery represents an unprecedented breakthrough in HIV research.
How mRNA Technology Works For HIV?
mRNA technology works by providing genetic instructions to cells, which in turn trigger them to make specific proteins. This was successfully employed in COVID-19 vaccines, allowing cells to produce viral proteins that educate the immune system.
In this HIV study, the mRNA causes infected white blood cells to display markers that indicate the presence of the virus. Basically, it "awakens" latent HIV in the cells so that current immune defenses and antiretroviral drugs can detect and eliminate the infection.
This strategy tackles one of the fundamental problems of HIV treatment—the elusiveness of the virus in reservoirs—and may signal a shift in treatment strategies.
Why is There A Global HIV Burden and the Urgency for a Cure?
Globally, there are almost 40 million individuals infected with HIV, out of which about 1.2 million reside in the United States alone. The current therapy includes daily antiretroviral therapy (ART) to suppress the virus, avoiding evolution into AIDS and transmission. ART is not a cure and is lifelong, though.
For all the strides that have been made in treatment and prevention, HIV still kills an estimated one person per minute worldwide, UNAIDS data as of 2023 indicate. It also continues to cause new infections, which intensify the need for a final cure.
Additionally, HIV disproportionately impacts vulnerable populations. In the United States, gay and bisexual men contribute to approximately 67% of new infections, a reflection of ongoing disparities and the need for creative solutions.
Though the breakthrough is groundbreaking, it is important to emphasize that this study is in its early stages. The experiments to date have been carried out in the laboratory, in cells from patients but not within the human body.
Before patients can benefit from this potential therapy, the treatment will need to pass through extensive tests in animal models to determine safety and efficacy, followed by strictly controlled human clinical trials. These procedures take years.
Dr. Cevaal warns against premature hope, recognizing that numerous biomedical improvements fail to reach clinical use. But she is optimistic: "In HIV cure, we have never seen anything as good as the way we're doing now, in terms of how well we can uncover this virus."
The new lipid nanoparticle delivery system could be used for conditions such as HIV treatment, but beyond it. According to Dr. Michael Roche, co-senior author of the research from the University of Melbourne, the targeted white blood cells are found in other conditions, such as cancers. This presents potential for mRNA treatments to revolutionize therapy for a range of conditions.
This finding not only demonstrates the strength of advanced biomedical research but also restores hope that an HIV cure, previously considered impossible, is within reach.
COVID-19 Cases In India Surges Past 5,000 With More Than 50% Affecting Adults Aged Between 25-50, State Officials Report

Credits: Health and me
India is witnessing a concerning surge in COVID-19 cases with active cases jumping over 5,364 as of June 7, as per the COVID dashboard, Ministry of Health and Family Welfare. The figure marks a sharp increase from only 257 active cases on May 22. More importantly, more than 50% of the new infections are in the 25-to-50-year age group the working population which has caused alarm among public health officials.
The number of new COVID-19 infections reported on a daily basis continues to slowly rise. On June 6, 564 cases were added in India, increasing the active caseload to 5,364. The number has now crossed 5,364, indicating an upward trend. Along with the increasing infections, at least seven fatalities were recorded within a 24-hour period, with the departed including those from West Bengal (4), Maharashtra (3), Delhi (2), Kerela (2) and Karnataka (3). All six of the seven deaths were older patients with comorbidities like diabetes, hypertension, or pneumonia. The youngest death was in a five-month-old male infant with pre-existing respiratory problems.
These new cases are caused, according to experts, by newly emerging subvariants such as LF.7, XFG, JN.1, and more recently identified NB.1.8.1. These variants are said to be more transmissible and have partial immune escape characteristics but, as of yet, have not shown increased disease severity.
Experts are seeing a trend towards mild to moderate symptoms, but the rate of infection is worrying as it is impacting the productive segment of the population and may stretch the healthcare machinery if not contained.
Kerala, Delhi, and Maharashtra Among Worst-Hit States
Kerala is still the hotbed of this new wave, with more than 1,487 active cases according to the latest report. Delhi (562), West Bengal (538), Maharashtra (526), and Gujarat (508) take second place. The Gujarat state has registered a high count of infections in the age group of 25-50 years, which has contributed to more than 50% of its 700+ total cases.
Surprisingly, officials also noted that around 10% of new cases in Gujarat were infants under the age of one. The elderly population, which bore the brunt of earlier waves, has seen relatively fewer infections in the current resurgence. This shift in demographic impact is being closely monitored by epidemiologists.
New COVID Symptoms To Note
In contrast to the previous waves where dramatic cases of anosmia (loss of smell) and ageusia (loss of taste) were observed, present patients are reporting a different constellation of symptoms. The most frequently reported symptoms are high-grade fever, intense muscle aches (myalgia), and gastrointestinal symptoms such as diarrhea.
This wave clinically is presenting differently. Patients, particularly those in younger age groups, are presenting with intense body pains and fever instead of respiratory complaints.
Hospitalization Rates and Deaths
Whilst the figure of cases is rising, hospitalization rates continue to be fairly low — ranging at about 5%. Nevertheless, the seven recent deaths serve as a stark reminder of the risk posed to vulnerable groups. Ministry data show all victims had comorbidities such as seizures, respiratory failure, kidney disease, and cancer.
Three of the recent Gujarat fatalities included young women aged 18, 20, and 47, all from Ahmedabad. "This is not common and highlights the need to not ignore any symptoms," said a senior health official.
The Indian government has sent advisories to every state and union territory in order to be prepared. This involves keeping proper stocks of oxygen, antiviral drugs, and ICU beds. States have also been instructed to distinguish between COVID-19 and other viral fevers, which have common symptoms.
A ministry senior official observed, "We are calling for all states to be on their toes and to intensify surveillance, particularly in urban areas and public transport hubs."
Hospitals and clinics in major metros are keeping a lookout, with training and testing protocols of the staff being revised to account for the evolving clinical presentation of the disease.
Vigilance Needed Even With Vaccination Efforts
India has come a long way in COVID-19 vaccination with more than 2.2 billion doses given so far, but the new variants have again pushed to the forefront the question of booster doses, particularly among frontline workers and the elderly.
Vaccination is not a static shield. As the virus mutates, so should our immunity. It's important to remain current with booster doses if they are suggested.
Although hospitalization and serious cases are still low, the recent spurt in COVID-19 cases in India is a stark reminder of how unpredictable the virus has been. With variants spreading and attacking younger people, a joint effort through vigilance, prompt testing, booster vaccinations, and responsible public action is a must.
For the time being, health authorities keep a close watch on trends, advising people not to ignore mild symptoms and to follow basic precautions such as hand hygiene, wearing a mask in crowded places, and seeking a test when symptomatic.
2 Infants Died Of Whooping Cough In Kentucky, Health Officials Report; Who Should Get A Booster Shot?
Two babies in Kentucky have lost their lives to pertussis, also known as whooping cough, as recently reported by the Kentucky Department for Public Health. These deaths, the first pertussis-related since 2018, have refocused attention on a resurging danger once thought largely brought under control in America- vaccine-preventable illnesses.
With over 10,000 cases reported across the country in the first six months of 2025, close to twice as many as the same six months a year ago public health officials are warning an alarm. The epidemic, which tracks with trends in other diseases like measles, coincides with declining childhood vaccination rates, anti-vaccination sentiment, and pandemic-period interruptions of routine vaccination activities.
Whooping cough is a very contagious respiratory infection that is brought on by the bacterium Bordetella pertussis, originally described in 1906 by French scientists. Nevertheless, centuries ago, there were mentions of the illness—its earliest probable epidemic was seen in Paris in 1578.
The disease is notorious for its intense, hacking cough that is followed by a piercingly high-pitched "whoop" upon inhalation. In newborns, particularly those too young to be vaccinated, pertussis may cause lethal complications such as pneumonia, seizures, and respiratory distress. Some doctors call it "the 100-day cough" because its duration lasts for many weeks or even months.
According to the World Health Organization, pertussis still causes approximately 160,700 deaths annually in children under the age of five worldwide, a statistic that highlights the ongoing global burden of the disease, especially in settings with limited vaccine coverage.
The two infants who perished in Kentucky in the last six months were not vaccinated, and neither were their mothers while pregnant. These events highlight a key gap in protection that maternal vaccination seeks to close. Babies under 6 weeks are too young to get their first dose of pertussis vaccine, and so remain extremely exposed early in life.
Third-trimester maternal immunization allows for the passing on of protective antibodies to the newborn, protecting them until they are of age to start their own vaccine regimen. Without the added layer of protection, there is a marked increase in risk of severe illness or mortality.
Through June 2025, the U.S. has reported a minimum of 8,485 confirmed cases of pertussis, already passing the 4,266 cases reported for the same period in 2024. For 2024, as reported by the CDC, a combined total of 35,435 cases were reported—more than five times that of 2023 and close to twice that of 2019, the final year before the pandemic.
Kentucky alone has reported 247 cases of pertussis through 2025, after reporting 543 cases in 2024—the largest number in the state since 2012. Across the country, from October 2024 through April 2025, four deaths from pertussis have been reported: two infants, one school-age child, and one adult.
Why Are Whooping Cough Cases Increasing Again?
The return of pertussis in the United States is being fueled by a mix of related factors. One major cause is the cyclical pattern of the disease, since pertussis has epidemic patterns with episodes peaking every two to five years. Although such peaks are anticipated, experts note that the current peak is more severe compared to what is normally seen during normal peaks. Post-pandemic immunity gap is also a crucial factor. Throughout the COVID-19 pandemic that occurred during 2020 and 2022, pertussis rates decreased significantly because of widespread public health interventions like masking, physical distancing, and closing schools. Since those measures are no longer in effect, numerous persons including children who were left unvaccinated or were missed during their periodic vaccinations since then are now at increased risk for infection. Adding to this problem is the decrease in vaccination coverage, driven by increased misinformation, increased skepticism about the vaccine, and interruptions in access to health care. That decline in immunization, especially in infants and pregnant women, is one of the most urgent priorities driving the national epidemic of pertussis.
How Effective Are Vaccines Against Pertussis?
The pertussis vaccine itself has changed dramatically over the years since it was first introduced in the U.S. in 1914.
Today's acellular form—DTaP for infants and children and Tdap for teens and adults—was introduced in the 1990s as a way to reduce side effects like seizures and high fevers that were caused by the older whole-cell vaccine. Although the acellular vaccine offers robust protection initially, the immunity fades with time. During the first year after completion of the five-dose course of childhood pertussis vaccination, some 98% of children are protected against pertussis.
By the fifth year after the last dose, however, that immunity declines to roughly 65%. This drop highlights the necessity of booster shots in young adulthood and adolescence to ensure sustained protection. While immunity from the current vaccine is not long-term, it still represents the best weapon against severe disease, complications, and mortality. The unvaccinated are 13 times more likely to develop pertussis compared to their vaccinated counterparts, and they have much greater risks of being hospitalized or killed by the disease.
Who Should Be Vaccinated, and When?
The CDC and other top public health organizations suggest:
Infants: Shots at 2, 4, and 6 months, with boosters at 15 months and 4 years.
Adolescents: A Tdap booster dose at 11 or 12 years.
Adults: One Tdap booster in adulthood, with re-vaccination every 10 years.
Pregnant Women: One dose of Tdap between weeks 27–36 of every pregnancy to confer immunity to the newborn through passive antibody transfer.
Local health departments might even suggest extra boosters for people who reside in outbreak-facilitating areas particularly on the West Coast, where states such as California, Washington, and Oregon have seen high case totals this year.
How Can You Protect Yourself and Your Family?
The increase in pertussis cases—and its disastrous effect on babies—underscores the necessity of public education, uniform messaging by health workers, and availability of immunization services. Parents and caregivers should be motivated to keep their own and children's vaccination schedules up to date, especially in communities where disease outbreaks are reported.
Clinicians have a key role in advising maternal immunization and informing families about the signs of whooping cough, which is likely to be confused with the common cold at its initial onset.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited