- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Explained: Your Seasonal Flu Shot Just Got Upgraded To A Nasal Spray Vaccine That Comes to Your Door

Credits: iStock
Flu season has meant rolling up your sleeve for a shot at the doctor’s office or pharmacy. Now, that’s changing. AstraZeneca has launched FluMist Home, the first FDA-approved flu vaccine that can be delivered to your doorstep and self-administered—no needles required.
This new option, a nasal spray version of the vaccine, builds on FluMist’s two-decade track record. First approved by the Food and Drug Administration (FDA) in 2003, FluMist has long been available at clinics and pharmacies. But in September 2024, the FDA gave the green light for at-home self-administration. Less than a year later, the program is rolling out across 34 states in time for the 2025–2026 flu season.
The stakes couldn’t be higher, last flu season was one of the most severe in recent memory. The CDC estimates up to 82 million illnesses, 1.3 million hospitalizations, and 130,000 deaths from flu between October 2024 and May 2025. Yet vaccination rates remained low, with fewer than half of Americans getting their annual shot.
Experts say that convenience is a major barrier. Between busy schedules, limited access to clinics, and vaccine hesitancy, too many people skip protection. FluMist Home could remove at least one of those hurdles by making the process as simple as ordering online.
“People are increasingly comfortable with managing their health at home—whether through Covid-19 tests or self-injections for chronic conditions,” explains AstraZeneca. “This option takes advantage of that shift and expands access to flu vaccination.”
Do's and Don'ts Of Using Flu Nasal Spray
FluMist Home is FDA-approved for people ages 2 through 49. Adults can use it themselves, while children as young as 2 can receive it with help from a parent or caregiver.
However, it’s not for everyone. Because FluMist is a live, weakened-virus vaccine, pregnant women and people with weakened immune systems should consult their doctors before considering it. Those outside the approved age range must still rely on traditional flu shots.
How FluMist Works?
The ordering process mirrors a telehealth experience. Patients complete a brief medical questionnaire online, which is reviewed by a licensed healthcare provider before the prescription is approved. Insurance covers the cost for most users, with a flat $8.99 shipping and handling fee.
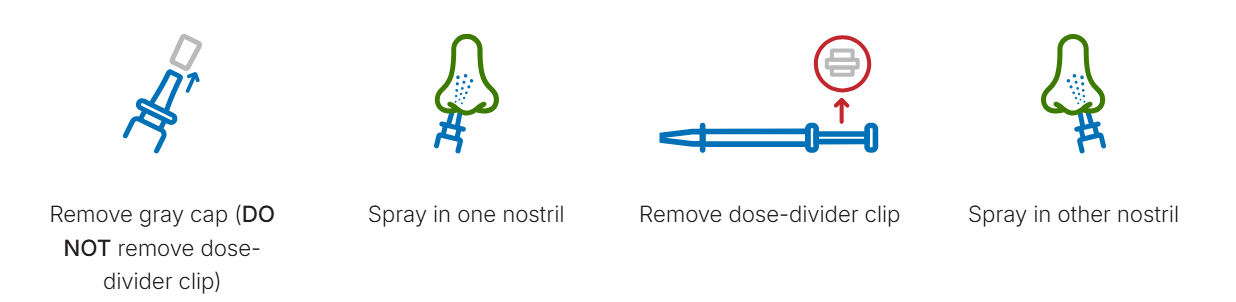
When FluMist arrives, it’s shipped in insulated, temperature-controlled packaging with ice packs to preserve stability. Each vial contains two pre-measured doses one for each nostril—separated by a clip. To administer, simply breathe normally while spraying; there’s no need to inhale deeply. A slight tickle, sneeze, or drip afterward is normal.
Patients can download a vaccination record from the online portal, and—if permission is given—the record is automatically shared with their doctor and uploaded to state vaccine registries.
Effectiveness and Safety
AstraZeneca emphasizes that FluMist Home uses the same formulation and vial as the version given in clinics. Its efficacy is on par with injectable flu vaccines, but the delivery method is needle-free.
The most common side effects are mild: runny nose, nasal congestion, and sore throat in adults. Children may experience low-grade fever. These symptoms generally resolve quickly.
Importantly, the FDA required AstraZeneca to conduct a usability study before approval. Results showed that 100% of participants were able to correctly self-administer the full dose without healthcare supervision.
How This Helps Tackle The Vaccination Gaps?
Needle-free, self-administered vaccines aren’t just about convenience—they may be critical in improving uptake. FluMist Home joins a growing trend of decentralizing preventive healthcare, putting tools directly into patients’ hands.
Historically, nasal spray flu vaccines were popular among children and adults who disliked shots. Now, offering a home option could further broaden access. As public health experts warn about the dangers of simultaneous flu, RSV, and Covid-19 waves, innovations like FluMist Home might play a pivotal role in reducing strain on hospitals.
The CDC notes that every additional percentage point increase in vaccination coverage can save thousands of lives during peak flu seasons. By lowering logistical barriers, FluMist Home could help close that gap.
Nasal Spray vs Shot: What Works Better?
The differences between FluMist and injectable vaccines come down to technology. Traditional flu shots use either killed viruses or specific proteins to teach the immune system how to respond. FluMist, by contrast, uses a live but weakened influenza virus. Both methods are proven to work, but some patients respond better to one than the other.
For people who avoid shots due to fear or discomfort, FluMist offers a gentler alternative. For children, especially, a quick nasal spray can mean less stress and higher compliance.
Could Nasal Sprays Be the Future of Vaccination?
The rollout of FluMist Home may be a harbinger of bigger changes. The pandemic normalized home-based care and accelerated acceptance of mail-order biologics, self-testing kits, and virtual consultations. Vaccines, once the exclusive domain of clinics, could follow suit.
Some researchers are already working on shelf-stable, oral, or patch-based vaccines that could one day make prevention even more accessible. For now, FluMist Home represents a significant step forward in modernizing how people protect themselves during flu season.
Useful Tips for Patients
Storage: Keep FluMist refrigerated (35°F to 46°F) until use.
Timing: Administer early in flu season for maximum protection.
Recordkeeping: Save your vaccination confirmation for medical records and travel purposes.
Disposal: Packaging materials are largely recyclable; chill packs can be reused.
FluMist Home gives people a practical, needle-free, at-home option to stay protected against the flu. While it’s not suitable for everyone, its convenience could boost vaccination rates at a time when respiratory viruses remain a major public health threat.
Shift to Plant-Based Proteins, Low-Fat Dairy To Boost Heart Health: American Heart Association

Credit: iStock
The American Heart Association (AHA), in its latest update on nutrition guidance, has urged the need to eat a diet rich in vegetables and fruits, while also making a key shift to plant-based protein from meat-based protein earlier to improve heart health.
It has also emphasized the need to reduce the intake of sugar, salt and ultra-processed foods, as well as to switch to low-fat dairy.
The scientific statement, which is issued about every five years, comes amid increasing cases of high blood pressure and obesity in the US, which can potentially lead to poor health outcomes, including deaths from cardiovascular disease and other chronic conditions.
“For healthy eating to be more attainable and sustainable, we recommend people focus on their overall eating pattern rather than specific nutrients or foods. This approach is actionable, something that can be modified as people pass through different life stages, while still adhering to the nine key features,” said Alice H. Lichtenstein, volunteer chair of the scientific statement writing committee and senior scientist.
“The guidance applies to wherever you eat: at home, school, work, restaurants, or in your community. You want to strive for progress rather than perfection. Every time you choose to make a swap for a healthier alternative, you’re making a step toward a healthier life,” added Lichtenstein, who is also senior scientist at the Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University in Boston.
The 9 Guidelines for a heart-healthy dietary pattern include:
- Maintaining a healthy body weight by balancing food intake and physical activity
- Eating plenty of vegetables and fruits
- Choose whole grains such as whole‑wheat bread, brown rice, and oatmeal over refined grains such as white bread or white rice
- Shifting from meat to plant-based sources such as legumes, including beans, peas, and lentils, along with nuts and seeds, and fish and seafood. Select low-fat or fat-free dairy products.
- Replace saturated fats with healthy unsaturated fats, including those from nuts, seeds, avocados, and non-tropical plant oils.
- Choose minimally processed foods instead of ultra-processed foods
- Limit beverages and foods with added sugars
- Choose foods low in sodium and prepare foods with minimal or no salt
- Limit intake of alcohol

Also read: AHA’s New Dyslipidemia Guidelines Stress Early Screening, Lifestyle Management
Healthy Eating Patterns From Childhood
The 2026 guidance for children recommends a heart‑healthy dietary pattern starting at 1 year of age. It urges families to play a significant role and become role models.
“Cardiovascular disease begins early in life; even prenatal factors can contribute to increased risk in children as they grow. So, it’s important that healthy eating patterns are adopted in childhood and continue throughout the entire lifespan,” Lichtenstein said.
“The best way to do that is for adults to role model heart-healthy eating patterns inside and outside the home,” she added.
Also read: Cardiovascular Diseases Lead As India’s Top Killer: US Cardiologist Points Out Risk Factors
While the updated guidance is specifically designed to improve cardiovascular health, it may also help improve other conditions like type 2 diabetes, kidney disease, some cancers, and brain health.
Breast Conservation Surgery vs Mastectomy: What Surgeons Recommend Today

Credit: Freepik
Breast cancer treatment has evolved significantly over the past few decades, moving from radical removal approaches to more personalized and tissue-preserving techniques. Today, surgeons no longer view breast conservation surgery (BCS) and mastectomy as competing options, but as equally effective strategies chosen based on individual patient needs.
With the growing availability of reconstructive surgery in Kolkata, patients now also have better cosmetic and psychological outcomes regardless of the surgical path they choose.
Understanding The Two Surgical Options
When faced with a breast cancer diagnosis, understanding the available surgical options is crucial for making an informed decision. Each approach is designed to effectively treat the disease while considering the patient’s long-term health, comfort, and quality of life.
What Is Breast Conservation Surgery (BCS)?
Breast conservation surgery, or lumpectomy or partial mastectomy, is a procedure that involves the removal of the tumor and a small amount of surrounding healthy tissue while preserving most of the breast.
The main objective is to remove cancer without altering the natural shape and appearance of the breast. Radiation therapy is usually administered after surgery to kill any remaining cancer cells and minimize the chances of recurrence.
What Is A Mastectomy?
Mastectomy is the removal of the whole breast tissue, and in other cases, the lymph nodes and skin around the breast. It can be done on either breast or both breasts based on the type of cancer and risk factors.
After a mastectomy, patients can choose to have breast reconstruction with the help of modern surgical procedures, such as those provided in reconstructive surgery in Kolkata, which can help to restore the shape and symmetry of the breast.
Major Differences Between BCS And Mastectomy
The basic distinction is the degree of tissue excision. BCS leaves the majority of the breast, but a mastectomy takes away all of it.
| Factor | Breast Conservation Surgery (BCS) | Mastectomy |
| Extent of Surgery | Removes tumor with a small margin of healthy tissue | Removes entire breast tissue |
| Invasiveness | Less invasive | More extensive surgery |
| Cosmetic Outcome | Preserves most of the natural breast shape | The breast is removed (reconstruction may be needed) |
| Recovery Time | Generally faster recovery | Longer recovery period |
| Radiation Therapy | Usually required after surgery | May or may not be required |
| Risk of Recurrence | Slightly higher local recurrence risk | Lower local recurrence risk |
| Hospital Stay | Often shorter or a day-care procedure | May require a longer hospital stay |
| Suitability | Early-stage cancer, smaller tumors | Larger tumors, multiple areas, or high-risk cases |
| Impact on Body Image | Better preservation of body image | May impact body image (can be improved with reconstruction) |
Notably, several studies indicate that both methods have equal chances of survival in the long term in early-stage breast cancer.
Eligibility Criteria: Who Can Opt For What?
Not every patient is suited for the same surgical approach, as the choice largely depends on individual clinical factors. Tumor size, stage, location, and overall health all play a crucial role in determining eligibility. Understanding who can opt for which procedure helps ensure both effective treatment and optimal long-term outcomes.
Candidates for Breast Conservation Surgery
BCS is usually prescribed to patients with:
- Stage I or II breast cancer
- Tumors smaller than 5 cm
- One tumor in one area
- No radiation therapy contraindications
- Some cases do not have high-risk genetic mutations like BRCA
It might not apply to patients who have more than one tumor in other parts of the breast or those with advanced disease.
Candidates for Mastectomy
Mastectomy may be suggested when:
- The tumor is huge in comparison with the size of the breast
- It has several tumors in various quadrants
- Cancer is metastatic (Stage III or IV)
- The genetic risk of recurrence is high in the patient
- Radiation therapy is not an option or choice
Moreover, other patients might opt to undergo mastectomy to have a sense of security or to alleviate the fear of recurrence.
Advancements In Breast Surgery
The current surgical advances have greatly enhanced the results, particularly in patients who want to preserve their breasts.
Oncoplastic Surgery
Among the most remarkable developments is the oncoplastic breast surgery that involves the use of both cancer resection and plastic surgery. This enables the surgeons to excise bigger tumors without altering the shape and symmetry of the breast.
This has increased the eligibility of BCS so that more women can avoid mastectomy and still have safe control of cancer.
Improved Imaging and Targeting
Modern imaging techniques have assisted surgeons in accurately identifying tumors so that they can be fully removed without damaging normal tissue. This enhances cosmetic outcomes as well as oncological safety.
Advanced Reconstruction Methods
The emergence of reconstructive surgery in Kolkata has given patients who have undergone mastectomy the opportunity to have an immediate or delayed reconstruction with the help of implants or autologous tissue.
Reconstruction has been brought to improve psychological well-being, body image, and quality of life.
Influencing Factors of Surgical Decision-Making
The decision to use BCS or mastectomy is not only a medical choice, but a very personal one, which depends on several factors:
1. Cancer Stage and Tumor Characteristics
The main determinants include tumor size, location, and spread. BCS is more appropriate in early-stage cancers, whereas mastectomy is usually necessary in advanced cases.
2. Survival and Recurrence Outcomes
It has always been demonstrated that the survival rates are the same with BCS (including radiation) and mastectomy in the case of early-stage cancers. Nevertheless, BCS can be slightly more likely to recur locally, which can be treated.
3. Patient Preference
A major role is played by emotional and psychological factors. There are those patients who want to keep their breasts, and others opt to undergo a mastectomy to have peace of mind. Studies show fear of recurrence is a major driver for choosing mastectomy.
4. Access to Radiation Therapy
Since BCS requires post-operative radiation, access to treatment facilities can influence the decision. Patients without easy access may opt for a mastectomy.
5. Cosmetic and Quality-of-Life Concerns
BCS tends to provide superior cosmetic results and satisfaction. Nevertheless, the modern methods of reconstruction have also helped to enhance the results of mastectomy patients considerably.
What Do Surgeons Recommend Today?
Modern breast surgeons support a multidisciplinary patient-centered approach. Instead of prescribing a single solution, they consider:
- Clinical (tumor size, stage, genetics)
- Access to care and patient lifestyle
- Motivational preparedness and individual interests
Surgeons are increasingly preferring breast conservation surgery in most of the early-stage cases because of its good results and quality-of-life advantages. Nevertheless, mastectomy is necessary in more complicated or risky cases.
Conclusion
The debate between breast conservation surgery and mastectomy is no longer about which is superior, but about which is most appropriate for the individual patient. Oncoplastic techniques and reconstructive surgery in Kolkata have advanced, and patients now have a choice of safer, more personalized, and cosmetically satisfying options.
The New Era of Cardiac Care: How Advanced Transplant Techniques are Saving Lives in India

Credit: Canva
Heart failure has quietly emerged as one of India’s most serious and underestimated health challenges, driven by a rise in hypertension, diabetes, obesity, and delayed diagnosis of heart disease.
Due to a shortage of donor organs and a long waiting period before receiving the right treatment, end-stage heart failure patients in India faced a lot of difficulties a few years ago.
Today, advancements in heart transplant techniques are changing the situation from what was once an untreatable condition to a second chance at life.
Data from the National Organ and Tissue Transplant Organization (NOTTO) shows a significant year-on-year rise in heart transplants, with 253 transplants done in 2024, showcasing improved organ donation awareness, better coordination between hospitals, and stronger transplant networks.
What was once considered the only option is now emerging as a life-saving solution, offering patients not just a second chance but a return to a more meaningful and active life.
Why Are Heart Transplants Needed?
A heart transplant offers hope and gives a second life to patients whose hearts no longer support the body even after the best available medical aid.
Although it is never performed instantly, it becomes necessary whenever conditions of the heart result in end-stage heart failure, where the pumping function of the heart is compromised.
Also read: Harish Rana’s Family Donated His Heart Valves And Corneas After His Death From Passive Euthanasia
When medications and modern technologies cannot supply an adequate amount of blood and oxygen to the organs, patients experience extreme breathlessness, fluid buildup, fatigue, and repeated hospitalizations, making even simple activities like walking, eating, or lying flat exhausting.
As the flow of blood continues to deteriorate, failure is also expected in other vital organs such as the kidneys and liver. It is at this point that the transplantation of the donor heart is considered the only treatment option to ensure that the blood flow is normalized.
How Heart Transplantation Transforms Life?
Heart transplant is not just a surgical replacement of a failing organ, but a complete life restoration for patients with end-stage heart failure.
Its benefits include:
- Normalizes Heart Functioning: A healthy donor heart can immediately restore normal and effective blood flow. This will reduce weakness and fatigue that makes carrying out everyday tasks rather difficult.
- Enhances Survival Rates: Patients diagnosed with end-stage heart failure can only experience the best post-transplant survival outcomes when they undergo the transplant procedure as compared to other medical treatments.
- Enhances Quality of Life: The patients are able to attain independence once again as they are able to walk, sleep, travel, and socialize with their families and friends.
- Prevents Frequent Hospitalization: The successful transplant procedure prevents constant hospitalization, especially in cases with deteriorating heart failure, infections, and organ dysfunction.
- Protects Other Vital Organs: By restoring adequate blood flow, heart transplantation helps reverse damage to the kidneys, liver, and lungs caused by prolonged heart failure
- Permits Return to Normal Roles and Responsibilities: Patients regain their ability to work, take care of others, and carry out their daily responsibilities, which helps their emotional well-being.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited