- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
2 Infants Died Of Whooping Cough In Kentucky, Health Officials Report; Who Should Get A Booster Shot?
Two babies in Kentucky have lost their lives to pertussis, also known as whooping cough, as recently reported by the Kentucky Department for Public Health. These deaths, the first pertussis-related since 2018, have refocused attention on a resurging danger once thought largely brought under control in America- vaccine-preventable illnesses.
With over 10,000 cases reported across the country in the first six months of 2025, close to twice as many as the same six months a year ago public health officials are warning an alarm. The epidemic, which tracks with trends in other diseases like measles, coincides with declining childhood vaccination rates, anti-vaccination sentiment, and pandemic-period interruptions of routine vaccination activities.
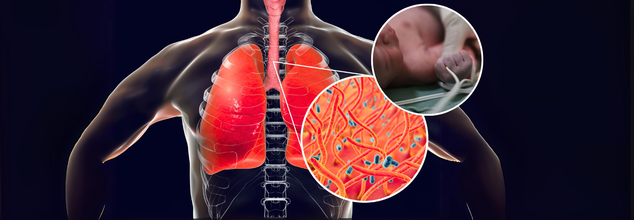
Whooping cough is a very contagious respiratory infection that is brought on by the bacterium Bordetella pertussis, originally described in 1906 by French scientists. Nevertheless, centuries ago, there were mentions of the illness—its earliest probable epidemic was seen in Paris in 1578.
The disease is notorious for its intense, hacking cough that is followed by a piercingly high-pitched "whoop" upon inhalation. In newborns, particularly those too young to be vaccinated, pertussis may cause lethal complications such as pneumonia, seizures, and respiratory distress. Some doctors call it "the 100-day cough" because its duration lasts for many weeks or even months.
According to the World Health Organization, pertussis still causes approximately 160,700 deaths annually in children under the age of five worldwide, a statistic that highlights the ongoing global burden of the disease, especially in settings with limited vaccine coverage.
The two infants who perished in Kentucky in the last six months were not vaccinated, and neither were their mothers while pregnant. These events highlight a key gap in protection that maternal vaccination seeks to close. Babies under 6 weeks are too young to get their first dose of pertussis vaccine, and so remain extremely exposed early in life.
Third-trimester maternal immunization allows for the passing on of protective antibodies to the newborn, protecting them until they are of age to start their own vaccine regimen. Without the added layer of protection, there is a marked increase in risk of severe illness or mortality.
Through June 2025, the U.S. has reported a minimum of 8,485 confirmed cases of pertussis, already passing the 4,266 cases reported for the same period in 2024. For 2024, as reported by the CDC, a combined total of 35,435 cases were reported—more than five times that of 2023 and close to twice that of 2019, the final year before the pandemic.
Kentucky alone has reported 247 cases of pertussis through 2025, after reporting 543 cases in 2024—the largest number in the state since 2012. Across the country, from October 2024 through April 2025, four deaths from pertussis have been reported: two infants, one school-age child, and one adult.
Why Are Whooping Cough Cases Increasing Again?
The return of pertussis in the United States is being fueled by a mix of related factors. One major cause is the cyclical pattern of the disease, since pertussis has epidemic patterns with episodes peaking every two to five years. Although such peaks are anticipated, experts note that the current peak is more severe compared to what is normally seen during normal peaks. Post-pandemic immunity gap is also a crucial factor. Throughout the COVID-19 pandemic that occurred during 2020 and 2022, pertussis rates decreased significantly because of widespread public health interventions like masking, physical distancing, and closing schools. Since those measures are no longer in effect, numerous persons including children who were left unvaccinated or were missed during their periodic vaccinations since then are now at increased risk for infection. Adding to this problem is the decrease in vaccination coverage, driven by increased misinformation, increased skepticism about the vaccine, and interruptions in access to health care. That decline in immunization, especially in infants and pregnant women, is one of the most urgent priorities driving the national epidemic of pertussis.
How Effective Are Vaccines Against Pertussis?
The pertussis vaccine itself has changed dramatically over the years since it was first introduced in the U.S. in 1914.
Today's acellular form—DTaP for infants and children and Tdap for teens and adults—was introduced in the 1990s as a way to reduce side effects like seizures and high fevers that were caused by the older whole-cell vaccine. Although the acellular vaccine offers robust protection initially, the immunity fades with time. During the first year after completion of the five-dose course of childhood pertussis vaccination, some 98% of children are protected against pertussis.
By the fifth year after the last dose, however, that immunity declines to roughly 65%. This drop highlights the necessity of booster shots in young adulthood and adolescence to ensure sustained protection. While immunity from the current vaccine is not long-term, it still represents the best weapon against severe disease, complications, and mortality. The unvaccinated are 13 times more likely to develop pertussis compared to their vaccinated counterparts, and they have much greater risks of being hospitalized or killed by the disease.
Who Should Be Vaccinated, and When?
The CDC and other top public health organizations suggest:
Infants: Shots at 2, 4, and 6 months, with boosters at 15 months and 4 years.
Adolescents: A Tdap booster dose at 11 or 12 years.
Adults: One Tdap booster in adulthood, with re-vaccination every 10 years.
Pregnant Women: One dose of Tdap between weeks 27–36 of every pregnancy to confer immunity to the newborn through passive antibody transfer.
Local health departments might even suggest extra boosters for people who reside in outbreak-facilitating areas particularly on the West Coast, where states such as California, Washington, and Oregon have seen high case totals this year.
How Can You Protect Yourself and Your Family?
The increase in pertussis cases—and its disastrous effect on babies—underscores the necessity of public education, uniform messaging by health workers, and availability of immunization services. Parents and caregivers should be motivated to keep their own and children's vaccination schedules up to date, especially in communities where disease outbreaks are reported.
Clinicians have a key role in advising maternal immunization and informing families about the signs of whooping cough, which is likely to be confused with the common cold at its initial onset.
AIIMS And ISRO Sign MoU To Advance Research In Space Medicine

Credits: Dr P Sarat Chandra (LinkedIn)
All India Institute of Medical Sciences (AIIMS) and the Indian Space Research Organisation (ISRO) signed a Memorandum of Understanding (MoU) on Monday to collaborate on advancing research in space medicine.
The MoU was signed between M Srinivas, Director (AIIMS), New Delhi and Dinesh Kumar Singh, Director, Human Space Flight Centre (HSFC), ISRO. The event brought together senior leadership from AIIMS and ISRO, including ISRO Chairman V Narayanan and Secretary, Department of Space, as well as Deans, Heads of Departments, faculty members, and studies from AIIMS New Delhi.
Also Read: Is There A Link Between Your Kidney Health And Other Chronic Diseases? Study Says Yes
As per the news agency Asian News International (ANI), a press release of the collaboration noted for a cooperative framework for ground-based and space-based research in Space Medicine. The press release also noted that the research will cover areas like human physiology, cardiovascular and autonomic regulation, musculoskeletal health in microgravity, microbiome and immunology, genomics and biomarkers and behavioral health.
“This MoU will give us the escape velocity to venture together into the field of space medicine. Collaborative research between AIIMS and ISRO will benefit patients, the nation, and ultimately humankind. As India moves toward Viksit Bharat by 2047, we hope to emerge as a Vishwaguru in space medicine as well,” said Prof M Srinivas, Director, AIIMS, New Delhi.

Chairman of ISRO Dr V Narayanan and Secretary, Department of Space also highlighted India’s remarkable journey in space programme. He noted how India evolved from the time when rockets and equipment were transported on bicycles and bullock carts to today, where it is going to be leading medical and research institutions like AIIMS to strengthen India’s human spaceflight capabilities.
The programme also featured a presentation on AIIMS New Delhi’s ongoing work in space medicine research, delivered by Prof. KK Deepak, former Head of the Department of Physiology. The event was attended by Heads of Departments and faculty members from across AIIMS New Delhi, along with representatives from the Resident Doctors Association (RDA), the AIIMS Student Association (ASA), and the Society of Young Scientists (SYS).
The collaboration represents an important step toward enhancing India’s capabilities in human spaceflight and biomedical research. It also aligns with the country’s broader scientific ambitions as India moves toward its centenary in 2047 and the vision of Viksit Bharat.
What Do We Already Know About Space Medicine?
As per a 2017 study in the British Journal of Anaesthesia, space medicine is fundamental to the human exploration of space. It supports survival, function and performance in this challenging as potentially lethal environment. It is international, intercultural and interdisciplinary, operating at the boundaries of exploration, science, technology and medicine.
Space medicine specialists play a crucial role in safeguarding astronauts and other spaceflight participants. Known as “flight surgeons,” they help develop strategies to protect the health, safety, and performance of space travellers in the extreme conditions of space. Their responsibilities span every stage of a mission — from selection and training to in-flight care, post-mission rehabilitation, and monitoring long-term health effects.
With inputs from ANI
Virus Without Vaccine Hits California; No Need To Worry, Say Public Health Officials
Credits: Canva
Sick days are again piling up with a respiratory disease, not COVID-19 or the flu. This disease is most likely the one Americans have not heard of. This is HMPV or human metapneumovirus. Doctors have asked people to stay vigilant as seasonal flu virus could lead to pneumonia and bronchitis, and it is spreading in California wastewater and around the country. However, as per public health officials, there is nothing to get worried at this point.
Also Read: Is There A Link Between Your Kidney Health And Other Chronic Diseases? Study Says Yes
As per the public database WasterwaterScan Dashboard, high levels of HMPV were detected across Northern California cities. The highest levels were reported in Redwood City, whereas elevated levels were found in San Francisco Bay Area and Napa's Wine Country. What's more dangerous is that this virus is without a vaccine.
The good news is that in other parts of country HMPV remains lower. However, the Centers for Disease Control and Prevention (CDC) noted that data from October 2025 shows the cases are trending up, especially during winter and spring.
Dr. Matthew Binnicker, director of the Clinical Virology Laboratory at Mayo Clinic, as reported by The Independent said, "In the late winter, early spring, it can account for five percent to 10 percent of all the respiratory infections that we diagnose in the United States. So it's definitely out there." Experts explain that other viruses like HMPV or influenza get a chance when COVID is quieter.
Read: HMPV Virus Cases Surging In California, New Jersey: Is It Dangerous?
Virus Without A Vaccine: What Is HMPV?
HMPV was first discovered in 2001 and is part of the Pneumoviridae family along with the Respiratory syncytial virus (RSV).
HMPV most likely spreads from an infected person to others through:
- the air by coughing and sneezing
- close personal contact, such as touching or shaking hands
- touching objects or surfaces that have the viruses on them, then touching the mouth, nose, or eyes
In the US, HMPV circulates in predictable patterns each year, typically beginning in winter and lasting through spring.
The usually self-limiting and mild symptoms typically last 4 to 5 days. These include:
- cough
- fever
- nasal congestion
- shortness of breath
People at risk include:
- elderly people
- children
- people with comorbidities
"The HMPV is not deadly, and there is no evidence of mortality or a severe transmission rate," former Indian Council of Medical Research (ICMR) scientist, Dr. Raman Gangakhedkar, told IANS, during the virus's outbreak in India in 2025.
“The virus may cause pneumonitis-like illness, but the mortality rates are almost unknown so far. HMPV has a global prevalence of about 4 per cent,” he added.
While no vaccine or treatment can prevent HMPV infection, to avoid the infection, individuals must:
Practice good hygiene and cover your mouth and nose with a tissue when coughing or sneezing, or use your elbow, not your hands, for it. And wash your hands properly, especially in healthcare settings.
Why Are People Hearing About The Virus Without Vaccine Now?
The reason people have not heard about it before is because its symptoms are nearly indistinguishable from other respiratory infections, so often it could go undiagnosed. Furthermore, earlier the COVID cases and influenza cases sparked up, which deviated the attention from HMPV. Now, with the season gone, and increased awareness around respiratory illnesses, greater attention to viruses like HMPV is also paid.
1 In 7 Indians Affected By Mental Health Disorders; Govt To Launch NIMHANS-2 To Boost Care

Credit: Canva
One in seven Indians, or over 14 percent of the population, suffers from some form of mental health disorder. Amid an increasing treatment gap -- up to 90 percent -- seen in several states, especially in North India, the government today reiterated the plan of launching a second National Institute of Mental Health and Neurosciences (NIMHANS) in the northern states.
NIMHANS-2 was first announced by Finance Minister Nirmala Sitharaman during the Union Budget 2026-27, to deliver specialized care for mental health and neurological disorders in north India.
Health experts and policymakers, as part of the government-led Post-Budget Webinar series, highlighted the growing burden of mental and neurological disorders in India and also stressed the urgent need to strengthen institutional capacity to meet emerging healthcare demands.
"One in seven Indians is affected by mental health disorders, while several states continue to face a treatment gap ranging from 70 to 90 percent," the experts said.
Noting that Non-Communicable Diseases (NCDs) account for over 60 percent of deaths in the country, they added that "neurological and mental health conditions are among the leading contributors to disability-adjusted life years (DALYs)," among the citizens.
Need For Tertiary Neuro-psychiatric Care
To address these, the experts called for ramping up tertiary mental health institutions and expanding specialized services.
The session, moderated by Vijay Nehra, Joint Secretary, Ministry of Health and Family Welfare, highlighted that North India currently lacks adequate tertiary neuro-psychiatric care facilities. These include areas such as:
- advanced neuroimaging,
- neurocritical care,
- specialized neurological services
Further, making a virtual address at the Post-Budget Webinar, Union Health Minister JP Nadda also highlighted the government’s focus on strengthening mental healthcare services in the country.
"NIMHANS-2 will be established in North India to expand advanced clinical care, training, and research," Nadda said.
"In addition, the Central Institute of Psychiatry, Ranchi, and the Lokopriya Gopinath Bordoloi Regional Institute of Mental Health, Tezpur, will be upgraded as regional apex institutions to strengthen mental healthcare services in the eastern and north-eastern regions," he added.
Meanwhile, the experts also stressed the need to improve services in underserved and geographically remote regions, including the northeastern states, through better infrastructure, capacity building, and targeted deployment of trained mental health professionals.
They also discussed strategies for expanding advanced neuro-psychiatric care and reinforcing India’s overall mental healthcare ecosystem. They proposed:
- Adopting a hub-and-spoke model supported by digital health platforms
This would allow tertiary institutions and centers of excellence to provide technical guidance, specialist consultations, and clinical support to district hospitals and community-level health facilities.
"Such a model would strengthen referral pathways and ensure that specialized mental health services are accessible to people even in remote and rural areas," the experts said.
- Integrating services under Tele-MANAS
Both existing and upcoming campuses of NIMHANS must be integrated , as this will enable a robust nationwide tele-mental health network that ensures
- timely counselling,
- psychological support,
- specialist consultations
- Digital follow-up systems
The experts called for the seamless integration of healthcare facilities, aligned with the vision of the Ayushman Bharat Digital Mission and the ABHA ID ecosystem. This, they said, will
- enable continuity of care,
- Improve monitoring of patients,
- Lead to better clinical outcomes
- A national Brain-Mind Cloud Network
The Network proposed under the National Health Mission would connect premier institutions such as All India Institute of Medical Sciences (AIIMS), state medical colleges, and primary healthcare centers through a digitally integrated platform.
It could also facilitate
- unified mental health records,
- AI-based screening tools,
- data-driven clinical decision support systems,
- tele-neuro-psychiatric hubs at regional centers.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited