- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Can AI Predict Your Risk Of Cancer? FDA Approved A New Tool That Spots Disease 5-Year Before It Appears
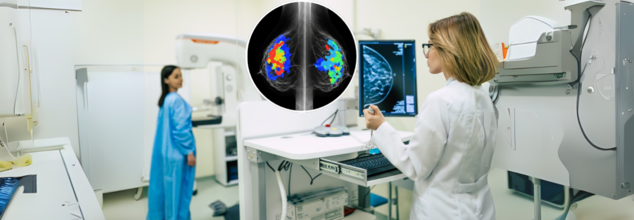
The U.S. Food and Drug Administration (FDA) has authorized the first-ever artificial intelligence (AI) tool designed to predict a woman’s five-year risk of breast cancer using a routine screening mammogram. The announcement, made on May 30, 2025by the tool’s developer, Clairity, marks a pivotal step in how breast cancer is detected and prevented—and it may just redefine the standard of care in women’s health.
This isn’t just another AI detection tool. Clairity’s platform, known as CLAIRITY BREAST, is not focused on spotting existing tumors, but rather on forecasting who may develop breast cancer years in advance. It shifts the paradigm from early detection to early risk prediction, potentially giving clinicians a critical head start in identifying high-risk individuals—before cancer ever forms.
This innovation comes from the vision of Dr. Connie Lehman, a radiologist and professor at Harvard Medical School, and the former chief of breast imaging at Massachusetts General Hospital. With decades of experience detecting cancers on mammograms, Lehman realized a key gap in screening: the lack of modern, image-based risk assessment tools.
“Our imaging technology was advancing fast, but our methods to identify women at high risk weren’t keeping up,” said Lehman at the 2025 American Society of Clinical Oncology (ASCO) Meeting, where the FDA authorization was announced.
While most existing risk models consider age, genetics, and family history, they often miss women who don’t fit those boxes. In fact, 85% of women diagnosed with breast cancer have no family history, and 50% have no identifiable risk factors at all. This makes Clairity’s approach uniquely valuable.
How The Breast Cancer Detection AI Tool Works?
CLAIRITY BREAST leverages deep learning and computer vision algorithms trained on millions of mammogram images, each linked to five-year follow-up data. By analyzing the subtle imaging features in breast tissue—often imperceptible to the human eye—the system generates a validated five-year risk score for each patient.
That score is integrated seamlessly into existing clinical workflows, providing radiologists and oncologists with a powerful new layer of information for decision-making.
“Now we can move even further upstream,” said Lehman. “Not just detecting cancer early—but predicting it, personalizing care, and even preventing it.”
Traditional screening strategies are reactive, catching cancer once it’s already present. But with Clairity, the approach becomes proactive, especially for women who may otherwise fall through the cracks of conventional risk models.
“This FDA authorization is a turning point,” said Dr. Larry Norton, founding scientific director at the Breast Cancer Research Foundation. “Most existing risk models miss the very women who go on to develop breast cancer. Clairity changes that.”
Younger women in particular stand to benefit. While breast cancer incidence is still highest in women over 50, cases among younger women are rising, yet they’re often not recommended for routine screening unless they have known risk factors. Clairity’s AI-powered insights can help clinicians tailor screening plans and intervene earlier for women who previously would have gone unflagged.
Dr. Lehman describes breast cancer not as a binary—either present or not—but as a continuum, with progression that begins long before a tumor is visible.
“There’s a point even before ductal carcinoma in situ (DCIS), when cancer hasn’t developed, but the risk is there,” she explained. “That’s where CLAIRITY can intervene—well before invasive cancer begins.”
The goal, according to Lehman, isn’t just to detect breast cancer earlier, but to predict and prevent it, in the same way that doctors routinely assess cardiovascular risk based on blood pressure, cholesterol, or BMI.
Until now, breast cancer lacked such a dynamic, image-based risk tool. That’s what makes Clairity’s authorization so significant.
AI’s Expanding Role in Radiology
AI has been used in radiology for decades, first to flag microcalcifications in mammograms in the early '90s. But back then, AI systems were limited to rule-based logic and needed exhaustive human guidance.
Today’s AI, especially in platforms like Clairity, goes far beyond what human vision can perceive. It identifies patterns in breast tissue texture and density at the pixel level, learning from vast image sets without needing explicit human-labeled inputs.
Lehman compared it to how machines learn to distinguish cats from dogs—by exposure to thousands of examples rather than being told what features to look for. In the case of breast cancer, the stakes are obviously much higher.
“This technology allows us to see what we couldn’t see before, and that opens doors to dynamic risk assessment,” Lehman said. “Eventually, we may even use these tools to monitor how interventions like medication, weight loss, or hormone therapy change a woman’s risk over time.”
Backed by Santé Ventures and ACE Global Venture, Clairity was founded in 2020 with a clear goal: to bring sophisticated AI tools to routine mammography. Now, with FDA de novo authorization, it’s set to hit the market by late 2025.
The company estimates the global market for breast cancer prediction tools at $63 billion, suggesting broad clinical interest and commercial potential.
As imaging centers, hospitals, and oncologists look to integrate risk prediction into daily care, Clairity's success will depend on adoption, clinician trust, and real-world outcomes. But with this regulatory milestone, a major hurdle has been cleared.
The FDA’s green light for CLAIRITY BREAST doesn’t just add a new tool to the cancer detection toolbox—it fundamentally changes the playing field. By enabling risk prediction from a single mammogram, it turns routine screening into a forward-looking, personalized roadmap for prevention.
Mystery Illness In Rajasthan Suspected To Be Viral Encephalitis: 2 More Children Dead
Credit: Canva
Two more children from Rajasthan's Salumbar district have fallen victim to the mysterious illness that officials now suspect to be viral encephalitis.
Since April 1, six children have died, including Deepak Meena (4), Seema (4), a one-year-old unidentified girl from Simor village, Laxman Meena (4), Kajal Meena (2), and Rahul Meena (4), within one or two hours of showing similar symptoms.
Also Read: Former US Senator Ben Sasse Opens Up About Battle With Terminal Stage 4 Pancreatic Cancer
According to health department officials, Raunak Ved (4) and Divyansh (2) were taken to a hospital on Wednesday evening after they developed high fever and vomiting.
“Soon after reaching the hospital, the doctor declared both of them dead. Although their symptoms were quite similar to those of the previous six cases, there were some differences in the pattern. It could be some different health issue, but we have yet to ascertain that. We have collected their samples and sent them for testing,” Salumber’s Chief Medical and Health Officer (CMHO), Mahendra Parmar, said.
With the additional cases, the death toll has gone up to 7 toddlers in Ghata and Lalpura villages.
Speaking to the media, Salumber’s district collector, Muhammed Junaid, said that two teams from the health department have been monitoring the situation constantly for the last few days.
“They have collected blood, stool, and saliva samples from children with suspected symptoms. Their samples have been sent to the National Institute of Virology (NIV) in Pune. We suspect it could be a kind of viral encephalitis, but we are yet to get the test report from NIV,” Junaid said.
All children reportedly experienced a sudden onset of fever that worsens rapidly, and claimed the lives of children within 24 hours.
The Health officials noted that at least 85 children were hospitalized with similar symptoms.
“The survey was conducted in 120,961 houses across the Udaipur division, during which over 940 children were found with similar symptoms. At least 75 of them were taken to a hospital. Anti-larval activity has also been carried out in 5,532 places after medical teams suspected viral encephalitis,” Junaid said.
What Is Encephalitis?
Encephalitis is the inflammation of the brain, caused by viral or bacterial infections, or by immune cells mistakenly attacking the brain.
People with encephalitis often show mild flu-like symptoms such as
- fever,
- fatigue,
- headache,
- body aches,
- confusion,
- seizures,
- changes in behavior or personality.
Types of Encephalitis
There are three main types of encephalitis:
- Viral or Infectious Encephalitis: It is the most common type of encephalitis that is caused by various viruses, including the West Nile virus, herpes simplex virus, Epstein-Barr virus, or varicella zoster virus. An individual may experience symptoms ranging from mild flu-like illness to severe neurological problems.
- Autoimmune Encephalitis: This is a rare condition where the body's immune system mistakenly attacks the brain cells due to a tumour or infection. While symptoms can vary widely, signs may include cognitive impairment, behavioural changes, and seizures.
- Bacterial or Fungal Encephalitis: While this type of encephalitis is less common, it can be life-threatening, especially for individuals with compromised immune systems. It may occur due to a complication caused by some other infections, such as meningitis. Symptoms can include high fever, severe headache, stiff neck, confusion, and seizures.
How To Prevent?
The risk of getting encephalitis can be reduced by protecting oneself from mosquito bites and staying up-to-date with vaccinations.
One must ensure getting vaccinated against mumps, chickenpox, measles, and rubella. The one-and-done vaccination, MMR vaccinations are given to people early in their childhood.
Flea-borne Typhus Surging Across Los Angeles, Officials Urge For Precautions

Credit: Canva
The Los Angeles County Department of Public Health has issued a warning about a surge in cases of flea-borne typhus, a bacterial infection transmitted by infected fleas, which are often carried by animals such as rats and cats.
In 2025, 220 cases were identified — the highest-ever recorded — with nearly 9 out of 10 requiring hospitalization.
Also Read: Encephalitis Alert In Rajasthan As Mystery Disease Claims 2 More Young Lives
While the disease needs more awareness and urgent prevention, the flea-borne typhus is treatable with antibiotics, especially when diagnosed early.
“Flea-borne typhus can cause serious illness, but it is preventable with simple steps,” said Muntu Davis, Los Angeles County Health Officer, in an official statement.
“With cases at an all-time high and most requiring hospitalization, it’s critical that people take simple steps now, such as routinely using flea control on their pets, avoiding contact with stray animals, and preventing wildlife from living in or around their homes,” Davis said.
The officials noted that people are often exposed in and around their homes when infected fleas are carried indoors on pets or other animals. Fleas that spread typhus are commonly found on stray animals, rodents, and other wildlife such as opossums.
The statement said that cases have been reported across Los Angeles County, including three localized outbreaks investigated in 2025 in Central Los Angeles City, the City of Santa Monica, and the unincorporated neighborhood of Willowbrook in South LA County.
“This marks a continued rise from 187 cases in 2024 and reflects a sustained upward trend in recent years,” it added.
Also read: Former US Senator Ben Sasse Opens Up About Battle With Terminal Stage 4 Pancreatic Cancer
Flea-borne Typhus: Symptoms and Treatment
Typhus is an acute febrile bacterial infection caused by Rickettsia Typhi bacteria, which is spread by infected fleas.
Because animals carrying infected fleas often appear healthy, people may not realize they are at risk.
Pets that spend time outdoors can carry fleas into homes and expose household members. People can also become infected through bites or feces of infected fleas, lice, or mites.
However, the flea-borne typhus is not spread from person to person.
The three main types—Epidemic, Murine, and Scrub typhus—all share common symptoms like high fever, headache, and rash.
Other symptoms of flea-borne typhus can include
- body aches
- muscle pain,
- nausea,
- vomiting.
"Some patients can develop severe illnesses in which multiple organ systems can be involved and really can result in death as well," said Medical Epidemiologist Dr. Aiman Halai with the Los Angeles County Department of Public Health, ABC7 reported.
Flea-borne typhus is treatable with antibiotics, and early diagnosis helps prevent severe illness and hospitalization.
The public health department in Los Angeles urged people to:
- Protect pets: Use flea control year-round
- Avoid stray animals: Don’t feed or handle them
- Keep wildlife out: Secure trash and block entry and hiding points.
Telangana Makes Cancer A Notifiable Disease: Why It’s Important?
Credit: Canva
In a significant move for public health, Telangana has declared cancer as a notifiable disease and launched a cancer registry.
The state reports about 55,000 to 60,000 new cancer cases every year.
A cancer registry would help the government in having accurate data for preparing better plans to deal with the spread of cancer, said the state Health Minister C Damodar Rajanarasimha.
He noted that the state government has expanded healthcare to treat cancer by establishing Day Care Cancer Centers in district headquarters towns. Further, the government is conducting health checks for 46 lakh members of women self-help groups (SHGs).
In addition, the government would also start Regional Cancer Centers and take measures to detect diseases like cancer through AI.
Is Cancer A Notifiable Disease In India?
A notifiable disease means that it is required by law to be reported to government authorities. The mandatory reporting facilitates surveillance, helps control.
Cancer is not currently a centrally mandated notifiable disease across all of India, as the central government focuses on surveillance through the National Cancer Registry Programme (NCRP). The NCRP was established in 1981 under the Indian Council of Medical Research (ICMR).
However, over 17 states and UTs in India have declared cancer a notifiable disease to improve data, registry accuracy, and early detection.
Also read: Cancer Is The 10th Leading Cause Of Death In Indian Children: Study
India operates two primary types of cancer registries to monitor the disease burden:
- Population-Based Cancer Registries (PBCRs): These collect data on all new cancer cases and mortality within a specific geographic area. Nearly 40 PBCRs are covering approximately 16.4 percent of India's population.
- Hospital-Based Cancer Registries (HBCRs) record information on patients diagnosed or treated at specific hospitals. There are currently over 269 HBCRs across the country.
“Cancer is emerging as a major public health problem in India. There is a need to collect accurate and robust data on cancer for planning optimal cancer care services across the country,” Dr (Prof) SVS Deo, Chairman – Surgical Oncology, Max Super Speciality Hospital, Saket, told HealthandMe.
The Role Of A Cancer Registry
Dr. Raghav Kesri, Senior Consultant & HOD, Medical Oncology, Yatharth Hospital, Greater Noida, said that cancer registration is significant in determining the types of cancers that are most common in a certain region.
It also allows us to pinpoint the risk factors that might contribute to the increasing number of cancer cases. In India, there are cancer registrations conducted by individual states and the country as a whole.
“These statistics allow us to analyze the trend when coupled with demographics, giving us important information to consider. This is critical knowledge to ensure that we go in the right direction in our health policies, including cancer prevention, early detection, and treatment,” Kesri told HealthandMe.
How To Prevent Cancers
Also read: Are Young Indians At Risk? The Rising Burden Of Early-Onset Cancers
Approximately 60 percent of cancers in India are preventable, including tobacco-related (lung and head and neck cancers), infection-related (stomach, liver, and cervical cancer), and lifestyle-related cancers (breast and colorectal cancers).
Common ways to prevent cancer include:
- Eating a healthy diet rich in fruits and vegetables
- Avoiding alcohol
- Quit smoking
- Avoiding tobacco consumption
- Stay physically active
- Maintain healthy weight.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited