- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
IBS Cases Surged During COVID-19 Pandemic, Study Finds
Credits: Canva
A 2022 study published in journal Frontiers in Medicine notes that there are about 10 to 23% of adults worldwide who suffer from irritable bowel syndrome (IBS). Another 2021 study that delves into the epidemiology of IBS and other bowel disorders of gut-brain interaction accounts for the global distribution of IBS by country in 26 countries that showed a high rate of consistency in prevalence rates. Among them was also the United States. Reflecting on the same data, a latest study published in the journal Neurogastroenterology & Motility notes that rates of IBS have nearly doubled among the US adults. It rose from 6% in May 2020 to about 11% in May 2022.
In the news release, the lead researcher Dr Christopher Almario, a gastroenterologist at Cedars-Sinai Medical Center in Los Angeles said, "Rates of digestive issues such as irritable bowel syndrome and chronic idiopathic constipation rose significantly."
“These findings underscore the significant toll the pandemic has taken on digestive health,” Almario added.
What Does The COVID-19 Pandemic Have To Do With IBS?
“These disorders involve chronic gastrointestinal symptoms that are often triggered or worsened by psychological stress,” Almario said.
It is no news that mental stress in fact increased during the COVID-19 pandemic. A report by the World Health Organization (WHO) indicated a 25% rise in the global prevalence of anxiety and depression in the first year of the pandemic. The National Institutes of Health (NIH) also notes that the pandemic's impact extended to vulnerable populations like adolescents, with increased suicidal ideation linked to infection fears.
Researchers also suggest that the rise in gut health disorders during the pandemic may be linked to both the impact of COVID-19 on the digestive system and the psychological stress caused by social distancing, isolation, and fear of infection.
Another study published in May 2020 in the United European Gastroenterology Journal noted that digestive diseases were amongst the most prevalent health conditions in Europe, as the study's area was focused in that very continent. The study noted: "OVID-19 has various implications on digestive health, as digestive symptoms such as nausea, diarrhoea and cramps occur in COVID-19 positive patients, in some cases, prior to respiratory symptoms. Moreover, people with chronic digestive conditions, including inflammatory bowel disease (IBD), digestive cancers, liver diseases or immunosuppressed liver transplanted patients, could be particularly vulnerable."
The study also noted that COVID-19 has demonstrated notable effects on digestive health. Studies indicate that the virus can impact the gastrointestinal tract and liver, with symptoms such as nausea, diarrhoea, and abdominal cramps. Elevated liver enzymes have been reported in up to 30% of patients.
Viral RNA has been detected in stool samples from 48.1% of patients, including those who tested negative via respiratory swabs. Digestive symptoms were present in 17.6% of cases, with incidence ranging between 5% and 50%. In some patients, gastrointestinal symptoms appeared before respiratory signs and were associated with more severe outcomes. Detection of the virus in stool suggests possible fecal-oral transmission, even from asymptomatic individuals.
Another 2021 study published in the journal Medicine Pharmacy Reports noted, "SARS-CoV-2 can affect major organs including the digestive system." The study reviewed other studies which have been conducted in UK, Wuhan, Hong-Kong, and America and have confirmed that while most common symptoms are fever, cough, and shortness of breath, other symptoms were also nausea, vomiting, abdominal pain, and diarrhea.
How Was The Study Conducted?
Researchers analyzed data from over 160,000 U.S. adults who took part in a national online survey conducted between May 2020 and May 2022. The survey collected information on digestive symptoms, mental health status, and lifestyle changes during the pandemic period.
Among participants diagnosed with irritable bowel syndrome (IBS), the most commonly reported subtype was mixed IBS, characterized by alternating episodes of both diarrhea and constipation.
“This research calls for a renewed focus on gastrointestinal health in the post-pandemic era,” senior researcher Dr. Brennan Spiegel, director of health services research for Cedars-Sinai, said in a news release.
What Are The Common Symptoms And Treatments Available For IBS?
The National Institute of Diabetes and Digestive and Kidney Diseases, US, notes the following as the symptoms of IBS:
- bloating
- the feeling that you haven’t finished a bowel movement
- whitish mucus in your stool
- diarrhea
- constipation
- women on their period will have more symptoms
IBS is typically treated through dietary and lifestyle changes, which are as followed:
- eat more fiber
- avoid gluten
- follow a special eating plan called the low FODMAP diet
- increasing your physical activity
- reducing stressful life situations as much as possible
- getting enough sleep
India To Strictly Inspect GLP-1 Drugs To Curb Misuse: Govt Flags Risks Amid Weight-loss Hype

Credit: iStock
GLP-1 drugs are powerful tools that can improve health, but it comes with risks and caveats. While these are medical therapies, they are being misused as cosmetic products by cosmetologists, physiotherapists, dermatologists, among others.
To curb its misuse and improve public health, the Indian government today issued guidelines on its use, while also flagging risks around it.
In an official statement issued today, the government has stated that it will roll out stricter inspections to curb the misuse of GLP-1 drugs in the country and will punish those who violate the rules.
“GLP-1 drugs are a significant medical breakthrough in treating type 2 diabetes and obesity, but they are not without risk. The drugs carry a wide range of side effects - from common symptoms like nausea and vomiting to severe complications including pancreatitis, kidney injury, and bowel obstruction. These risks make it essential that GLP-1 drugs are only taken under the supervision of registered medical practitioners/specialists,” the statement said.
In the wake of its hype over weight loss, the country's regulatory authorities have taken firm steps to prevent unsupervised use and malpractices in the supply chain.
It has “strongly advised” patients and the public to” consult a qualified medical specialist before use, and to obtain these medications with prescription only through legitimate, regulated channels”.
“Stricter inspections and surveillance will continue in the coming weeks. Businesses that break the rules will face license cancellation, fines, and legal action,” the statement said.
Also read: GLP-1 Drugs: Why India Needs Stricter Rules Now
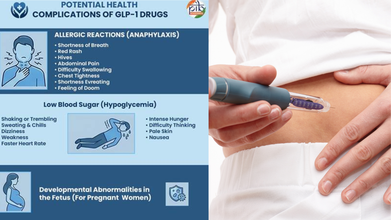
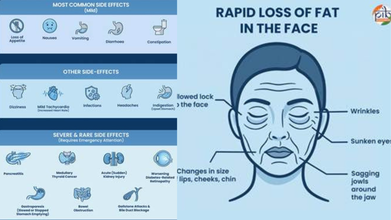
What Are The Side-effects Of GLP-1 Drugs?
GLP-1 drugs work to keep food in the digestive system for longer – making people feel fuller for longer, thus reducing appetite and inducing weight loss. Hence, the drugs are also prescribed to people with obesity.
However, when done without clinical oversight, it can lead to severe health complications.
There are various side effects to taking GLP-1 drugs, including nausea and dizziness, to pancreatitis and medullary thyroid cancer.
Some serious side effects include
- Pancreatis
- Thyroid Cancer
- Acute (Sudden) Kidney Injury
- Worsening Diabetes-Related Retinopathy
- Gallstone & Bile Duct Blockage
- Rapid loss of fat in the face
- Wrinkles
- Sunken eyes
GLP-1 medications may also complicate various health conditions, such as allergic reactions, with shortness of breath and low blood sugar.
Rush For Generic Weight Loss Drugs
The government's advisory comes as patent for semaglutide -- an active ingredient in diabetes and anti-obesity drugs, specifically Wegovy and Ozempic -- expired on March 20.
This has led to a rush among Indian pharma companies to launch cheaper generic versions, significantly increasing affordability and access for millions battling Type 2 diabetes and obesity.
Also read: CDSCO threatens action against pharma companies for promoting GLP-1 weight-loss drugs
Major Indian drugmakers who launched their generic semglutide injection in the country in March include Sun Pharmaceutical Industries, Zydus Lifesciences, Alkem Laboratories, and Dr. Reddy’s Laboratories.
WHO Guidelines on GLP-1 drugs
Amid the increasing prevalence of GLP-1 drugs, the World Health Organisation (WHO), late last year, acknowledged its role in treating obesity.
However, it warned that medications like GLP-1 alone will not solve the problem affecting more than one billion people worldwide.
The global health body also issued conditional recommendations for using these therapies as part of a comprehensive approach that includes healthy diets, regular physical activity, and support from health professionals.
Ozempic And Wegovy Prices Slashed Again In India To Counter Cheaper Generics

Credit: iStock
Danish pharma giant Novo Nordisk has once again reduced the prices of its blockbuster drugs Ozempic and Wegovy in India. The strategic move is aimed at staying ahead of the entry of the low-cost generic competition in the country.
Starting today, the Ozempic price in India will be cut by 36 percent, while Wegovy has seen a steeper 48 percent reduction — limiting the base price below Rs 6,000 per month.
While Ozempic is available in three dose strengths of 0.25 mg, 0.5 mg, and 1 mg in India, Wegovy has five dose strengths.
Ozempic's and Wegovy's lowest doses of 0.25 mg will now be priced at Rs 1,415 for a weekly shot from Rs 2,200 and Rs 2,712 earlier, respectively, Novo Nordisk India said in a statement on Tuesday.
The average price reduction across doses is 23.8 percent for Ozempic and 27 percent for Wegovy, it added.
Speaking to the media, Novo Nordisk stated that the price cut will benefit a large section of people with diabetes and obesity in India.
The generic weight loss drugs will open up a huge customer base, especially in India, with a high burden of diabetes and obesity.
Novo first slashed Wegovy's price for the first time by up to 37 percent from its launch price last year.
In addition to the entry of generics, the launch of rival Eli Lilly's blockbuster diabetes and obesity drug Mounjaro in India in 2025.
Also read: Semaglutide Becomes Cheap In India: A Gamechanger Or Health Gamble?
Entry Of Generics In India
Soon after the end of Novo Nordisk's patent on semaglutide, on March 20, a host of companies in India launched generic versions of Ozempic.
This includes NATCO Pharma's Semanat and Semafull, priced at Rs 1,290 per month and Rs 1,750 — about 90 per cent cheaper than Ozempic, costing Rs 8,800 per month.
Eris Lifesciences also announced its plans to launch a multi-dose vial under the brand name Sundae at the same price.
Dr. Reddy’s Laboratories, Sun Pharmaceutical Industries, and Glenmark Pharmaceuticals have also launched their generic versions of semaglutide.
Dr. Reddy’s Obeda is priced at Rs 4,200 per month, available in 2 mg and 4 mg strengths.
Sun Pharmaceutical Industries will sell under the brand names Noveltreat (doses ranging from Rs 900) and Sematrinity (doses ranging from Rs 750). Meanwhile, Glenmark’s GLIPIQ vials range from Rs 325 to Rs 440 per week.
Zydus Lifesciences has also announced the launch of its generic version of semaglutide injection under the brand names SEMAGLYNTM, MASHEMATM, and ALTERMET. The average monthly cost of the treatment will be about Rs 2,200, the company said in a statement.
How Does Semaglutide Work?
Semaglutide works as a GLP-1 receptor agonist that mimics the GLP-1 hormone to regulate appetite and blood sugar. It slows gastric emptying and makes you feel fuller longer. It also signals the brain to reduce hunger and cravings, and triggers the pancreas to release insulin when blood sugar is high.
Also read: This Pill Is More Effective For Weight Loss Than Ozempic, Scientists Say
They work by increasing insulin release in a glucose-dependent manner, decreasing the liver's production of glucagon, and slowing down the emptying of the stomach, which helps lower blood sugar levels after a meal. They also act on the brain to suppress appetite and increase feelings of fullness, leading to reduced calorie intake.
In people with type 2 diabetes, notes Harvard Health, the body's cells are resistant to the effects of insulin and the body does not produce enough insulin, or both. This is when GLP-1 agonists stimulate the pancreas to release insulin and suppress the release of another hormone called glucagon.
These drugs also act in the brain to reduce hunger and act on the stomach to delay emptying, so you feel full for a longer time. These effects can lead to weight loss, which can be an important part of managing diabetes.
Leptospirosis: US health officials flag outbreak risk after floods in Hawaii
Credit: iStock
Health officials in the US have issued a risk of leptospirosis — a bacterial illness — in Hawaii, after the “Kona low” storm floods.
The Hawaii Department of Health (DOH) and the Hawaiian Humane Society (HHS) have urged residents and recovery workers to monitor for signs of leptospirosis that can affect both people and pets.
Leptospirosis is caused by bacteria Leptospira, which are carried in the urine of infected animals, including rats, mice, mongoose, livestock, and dogs.
The disease can spread via the urine of infected animals and can enter the human body through broken skin or through the mouth, nose, or eyes.
“Hawaii already has among the highest rates of leptospirosis in the country due to its warm, wet climate,” said HHS and DOH in a joint statement.
“Flooding events like the recent Kona low storm can dramatically increase exposure risk by spreading contaminated soil and water across a broad area,” it added.
The agency urged people to check out symptoms in pets, such as fever, decreased appetite, vomiting, diarrhea, and muscle soreness, and get medical help.
The risk of Leptospirosis outbreak is common after a storm, because the dead animals are likely to spread the bacteria. Further, flooding also forces rodents out of their burrows, leading them into homes, shelters, and debris piles where they shed bacteria more easily.
What Is Leptospirosis?
Leptospirosis is one of the most prevalent zoonotic diseases worldwide, often linked to poor sanitation and agricultural practices that involve contact with animals or contaminated water.
The bacteria can survive in contaminated water or soil for weeks to months, primarily spreading through the urine of infected animals.
Humans can contract the disease through direct contact with infected urine or through contaminated food, water, or soil.
There are two main forms of leptospirosis: icteric leptospira, which presents with jaundice, and anicteric leptospira, a milder variant without jaundice. Leptospirosis can also manifest as Weil's disease, a severe complication.
What Are Symptoms Of Leptospirosis in humans?
Symptoms typically develop 2 to 30 days after exposure and can range from mild to severe. Initial signs often include
- high-grade fever,
- red eyes (conjunctival suffusion),
- calf tenderness,
- headache,
- dry cough,
- nausea,
- diarrhea.
In more serious cases, the infection can lead to complications such as
- jaundice,
- kidney damage
- liver damage,
- meningitis,
- respiratory issues,
- hemorrhages.
Pulmonary hemorrhage — acute bleeding from the lungs — can also occur, posing life-threatening risks such as respiratory and renal failure. The illness may last from a few days to several weeks, and without treatment, recovery can take months, according to the US Centers for Disease Control and Prevention (CDC).
What Precautions Should Be Taken?
To reduce the risk of leptospirosis infection, individuals are advised to take several important precautions. According to the CDC, it is essential to avoid wading through dirty rainwater, especially during the rainy season, and to wear gumboots in such conditions.
Proper care of any injuries or cuts is crucial, and frequent handwashing, particularly after handling food or working in potentially contaminated environments, is highly recommended. Additionally, individuals should avoid contact with animals that appear sick or are known carriers of the bacteria.
Vaccination is also vital—pet owners should ensure their pets are vaccinated against leptospirosis, especially if they are frequently exposed to water or wildlife. Staying hydrated by drinking plenty of clean water and preventing water stagnation around the home can further minimize the risk of infection.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited