- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Jason Kelce Says He ‘Virtually Guarantees’ He Has CTE; Know All About The Brain Disorder You Can Only Diagnose After Death
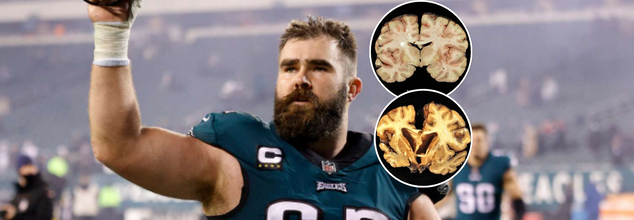
Philadelphia Eagles legend center Jason Kelce recently shared that he "virtually guarantees" that he has chronic traumatic encephalopathy (CTE). Kelce's statement, posted on social media in answer to an argument, was blunt and stark, the NFL star sais, "All the research would suggest I have some degree of it." The veteran player's remarks aren't baseless because recurrent head trauma, a sad reality of high-impact sports such as football, is directly associated with CTE—a degenerative brain illness that, until death, may not be diagnosed.
This discovery isn't limited to one competitor—it represents a broader issue for athletes, families, coaches, and the medical establishment.
What Is CTE?
Chronic Traumatic Encephalopathy (CTE) is a brain disorder thought to be caused by repeated head trauma. It can involve concussions and even subconcussive blows that do not have any immediate symptoms. Although CTE was initially diagnosed in boxers during the early 20th century, it is now most famously linked with professional football players, military combat veterans, and contact sports athletes.
What's most concerning about CTE is its subtlety: the disease develops in silence, and existing technology is unable to detect it in the living. It can only be conclusively identified by postmortem brain autopsy. While uncommon in the general population, CTE is at shockingly high prevalence among retired NFL players and others with chronic repetitive head trauma.
Jason Kelce's frankness is remarkable. Though healthy and active, he is aware of the probability of contracting a disease whose symptoms can take years to materialize after retirement. "Although there is no test to determine if I have CTE at the moment, the evidence points to me probably having it," Kelce wrote. This kind of candor brings the long-term costs of professional sport into sharp focus, especially for linemen like Kelce who are subject to helmet-to-helmet collisions day in and day out.
His words can be bleak, but aren't intended to be shocking—they're a wake-up call. They force the greater athletic community to grapple with uncomfortable realities regarding brain health, risk, and the cost of performance.
How CTE Develops Over Time?
Unlike what most people think, CTE is not brought on by one traumatic event. Rather, it's linked to a history of repeated blows to the brain during a period of time. That means both concussions and lesser blows that do not always have readily apparent symptoms. They can build up and gradually initiate neurodegeneration.
Eventually, this damage causes an accumulation of a misshapen protein known as tau, which moves from cell to cell within the brain, causing cells to die and function to be impaired. The resulting injury harms mood, thinking, and motor function, making daily life more and more challenging.
What Are the Symptoms of CTE?
While CTE cannot be diagnosed in the living, physicians are frequently able to identify a condition called traumatic encephalopathy syndrome, which shares many of the same symptoms. Some of these include:
Cognitive Impairment: Concentration difficulties, loss of memory, and problems with planning or organizing.
Behavioral Changes: Aggression and impulsivity, frequently misinterpreted as personality defects.
Mood Disorders: Ongoing depression, emotional instability, substance abuse, and even suicidal ideation.
Motor Impairments: Walking difficulties, tremors, speech problems, and Parkinson's disease-like symptoms.
Notably, not all repeated head trauma victims will develop CTE—but the likelihood of it is greatly increased with the number of injuries incurred.
Challenge of Diagnosing CTE During Life
One of the most infuriating parts of CTE is that it cannot be diagnosed conclusively until after death. Although researchers are developing possible biomarkers that could be used to detect CTE in the living, none of these have been confirmed yet. This means those at risk, such as professional athletes, fall into a medical twilight zone where symptoms are not taken seriously or are wrongly assigned.
CTE continues to be an underestimated and not well understood condition. Never has increased awareness, improved diagnostic methods, and long-term research funding been more vital.
Although there is no cure for CTE, there are steps that can be taken by athletes, organizations, and families to lower risk and assist those who are suffering:
Education and Awareness: Familiarity with signs of concussion and referral for medical assessment following head trauma can avoid further injury.
Changes in Play: Football and other contact sports are modifying to limit head trauma with rule adjustments, equipment development, and tackling styles.
Mental Health Resources: Individuals presenting with mood or cognitive changes need professional intervention early on. Depression and suicidal ideation are concerning issues that can and should be addressed.
Monitoring and Support for Retired Athletes: Periodic neurological testing and frank discussion can facilitate former players taking charge of their health.
Jason Kelce's blunt comment about CTE can be a strong legacy—not as a great player, but as a force for transformation. By accepting the probable truth of brain damage, Kelce is taking the conversation in a new direction and inviting others to fight for safer play, improved treatment, and greater knowledge.
His voice adds to an increasing chorus of athletes and medical professionals demanding real change in the way that we do sports, health, and long-term brain safety. And until we can perhaps reverse CTE, discussions like these at least make sure that we are no longer turning a blind eye to it.
Cicada COVID Variant: Use Masks To Avoid Transmission, Say Experts

Credit: Canva
The emerging COVID variant, BA 3.2, nicknamed “Cicada,” has revived memories of the COVID-19 pandemic that disrupted the world and raised fresh concerns about the possibility of severe illness.
The variant has been given the nickname “Cicada” due to its reappearance after remaining dormant or undetected for a long period, much like cicadas that emerge after years underground.
With the variant already spread to 23 nations, as of February, experts are urging people to use masks to avoid transmission.
What Is The Cicada COVID Variant?
Cicada was first identified in a respiratory sample in South Africa in November 2024.
It is a descendant of the Omicron BA.3 lineage, and is genetically distinct from the previously circulating JN.1 lineages (including LP.8.1 and XFG).
BA.3.2 comprises two major branches, BA.3.2.1 and BA.3.2.2. BA.3.2.2 also has substitutions like: K356T, A575S, R681H, and R1162P.
The World Health Organization (WHO) has designated BA.3.2 as a Variant Under Monitoring (VUM). It means the variant may not be that dangerous yet, but it may have concerning mutations.
As per the US CDC’s latest Morbidity and Mortality Weekly Report, Cicada has “70 to 75 substitutions and deletions in the gene sequence of its spike protein”.
Time To Mask Up
Dr. Sai Balasubramanian, a doctor and healthcare strategy executive, writing in Forbes, stressed the need to follow COVID practices such as masks and hand hygiene.
"Healthcare professionals recommend taking general precautions, similar to those used to prevent most viral transmission: get vaccinations when appropriate, wear masks in crowded areas or indoors where there is a high risk of transmission," he said.
He also urged “avoid individuals who have known illness or infections, wash hands frequently, and continue to stay apprised of local community guidelines and the infection spread”.
Cicada variant “is different from the (Covid-19) viruses we have been dealing with for the last two years," Prof Ravi Gupta, of Cambridge University, who advised the UK government during the pandemic, was quoted as saying by The Mirror.
Will The Cicada Variant Cause Severe Illness?
The SARS-CoV-2 virus has the potential to turn deadly in people, especially among vulnerable populations such as those with a weak immune system.
The Cicada variant is particularly concerning as it provides no immune protection to people with previous infection or even vaccination.
Yet, the World Health Organization and health experts advise that existing COVID vaccinations can help prevent severe illness and hospitalization.
"It would appear that all the protections we have from our experience with the virus and with vaccines probably offer more limited—not zero—but more limited protection against this strain," Dr. William Schaffner, professor of infectious diseases at Vanderbilt University Medical Center, was quoted as saying by Time.
Cicada Variant: Any New Symptoms?
The symptoms of Cicada aren't different from those of previous COVID variants. These include:
- sore throat,
- fever or chills,
- headache,
- cough,
- body aches,
- runny nose
- nausea
- diarrhea.
Tpoxx Should No Longer Be Used For Treating Mpox: European Drug Regulator

Credit: Canva/ US CDC
The European Medicines Agency (EMA) has advised patients and physicians not to use the antiviral drug Tecovirimat SIGA (marketed as Tpoxx) to treat mpox disease.
The advisory from the EMA’s Committee for Human Medicines (CHMP) is based on data from four studies carried out in different regions, which showed that compared with placebo treatment with Tpoxx did not
- heal lesions faster
- relieve pain
- help clear the virus from the body faster.
“The animal data demonstrated antiviral activity and a survival benefit when treatment was started early and a reduced efficacy if treatment was initiated later after exposure to the virus,” the EMA said in an official statement.
However, the clade 2 mpox outbreaks, which began in 2022, led the World Health Organization (WHO) to declare mpox a Public Health Emergency of International Concern (PHEIC), giving the drugmaker SIGA Technologies an opportunity to conduct efficacy studies in people.
A second PHEIC was declared in 2024 over clade 1 outbreaks.
Key recommendations by the EMA include:
- Restricting the use of Tpoxx over no benefit.
- Due to lack of safety concerns, patients who initiated treatment with Tpoxx can continue till course ends.
- Tpoxx can still be used as an antiviral to treat other orthopoxvirus infections, including smallpox and cowpox
- There is currently no other drug authorized in the EU for treating mpox infections.
Tpoxx For Mpox: What Does The US CDC Say
The Centers for Disease Control and Prevention also noted that the role of Tpoxx in treating mpox "is investigational".
The federal agency called for "additional clinical trials" to explore the role of Tpoxx in treating mpox infections in patients with severe immunocompromise, including advanced HIV.
"The findings from the clinical trials suggest that most patients with monkeypox who do not have severe disease or risk factors for severe disease (e.g., severe immunocompromise) will recover with supportive care and pain management," the CDC said.
Also read: Missouri Reports 2 Cases Of Deadly Clade I Mpox, US Tally Rises To 3 In 2026
What Is Mpox?
Mpox, earlier known as monkeypox, is a rare viral disease that belongs to the orthopoxvirus genus, the same family as the more well-known smallpox virus.
Though generally less severe, mpox can still lead to serious health complications, especially in immunocompromised individuals, children, and pregnant women.
The virus is transmitted from animals to humans and can spread from person to person through direct contact with infectious sores, scabs, body fluids, respiratory droplets, or contaminated materials.
Also read: Mpox Outbreak: First Case of Severe Strain Reported in New York City
The earliest signs of mpox start within 14 days of being infected. A person may not know they have mpox and can spread the disease.
The common symptoms include:
- fever,
- sweating,
- chills through the body.
- rashes, which start as a distant rash on the face and can continue throughout the body,
- swollen lymph nodes, migraine,
- muscle aches,
- fatigue,
- weakness
- back pain.
Mpox: Current Cases
In February, a total of 1,184 confirmed mpox cases and four deaths were reported from 46 countries, as per the WHO's latest outbreak update.
Of these cases, 58.6 percent were reported in Africa — mainly from Madagascar, the Democratic Republic of the Congo, Kenya, Burundi, and Liberia.
The WHO said all clades continue to circulate, and transmission of the virus continues mostly within sexual networks, followed by household transmission. All age-groups in some historically endemic areas are being affected.
“Unless mpox outbreaks are rapidly contained and human-to-human transmission is interrupted, there is a risk of sustained community transmission in all settings,” the WHO said.
Study Shows Ebola Virus May Persist In Breast Milk For Over 3 Months After Recovery
Credit: Canva
Even after recovery, the deadly Ebola virus (EBOV) can persist for a longer duration — more than three months — in breastmilk, according to a case report.
Ebola virus disease (EVD) is a severe viral illness that has a 25 percent – 90 percent fatality rate.
Ebola in pregnancy raises significant complications ranging from spontaneous abortion to maternal and neonatal death.
In a case report published in the New England Journal of Medicine, a team of researchers from the Republic of Congo and Senegal shared the case history of a 23-year-old woman in whom Ebola was still detectable in breast milk at 14 weeks.
The case reported the rare occurrence of a pregnant woman who survived EVD with no complications, neither to the mother nor the baby. However, the deadly virus was still present in the mothers' breast milk, which cited the potential risk of post-illness transmission to infants.
What Is Ebola Virus Disease?
As per the World Health Organization (WHO), EVD is a rare but severe illness in humans and is often fatal.
People can get infected with the virus if they touch an infected animal when preparing food, or touch body fluids of an infected person such as saliva, urine, feces or semen, or things that have body fluids of an infected person like clothes or sheets.
Ebola enters the body through cuts in the skin or when one is touching their eyes, nose or mouth. Early symptoms include fever, fatigue and headache.
What Was The Case
The woman from the Democratic Republic of the Congo (DRC) contracted EBOV during pregnancy in 2019.
Soon after, she was administered monoclonal antibody therapy and was discharged after three negative reverse-transcriptase–polymerase-chain-reaction blood tests for EBOV.
The woman delivered a healthy baby at 42 weeks of gestation. No evidence of EBOV infection was found in maternal blood, amniotic fluid, vaginal secretions, or the newborn.
Ebola Detectable In Breast Milk At 14 Weeks
Yet surprisingly, the EBOV virus persisted in the placenta and breast milk.
Tests revealed that while the mother’s blood remained negative, viral RNA was still detectable in breast milk at 14 weeks after illness onset. To protect the newborn from transmission, clinicians used the drug bromocriptine to suppress lactation.
As per the World Health Organization (WHO) guidelines, the mother was also isolated from the baby and not breastfed. A prophylactic (preventive) monoclonal antibody was also given to the newborn. During follow-up, the infant exhibited no signs of infection.
Ebola Virus: WHO Guidelines
During the 2018–2020 EVD outbreak in the northeast of DRC, 3,481 confirmed cases were reported. Of these, nearly 60 percent occurred in females, and about 45 percent occurred in children below 18 years of age.
Current WHO guidance recommends that Ebola survivors avoid breastfeeding until viral clearance is confirmed.
The global health body advises women with suspected or confirmed Ebola to immediately stop breastfeeding and be prioritized for diagnostic testing.
Children exposed to Ebola through breast milk
- Must be placed under care,
- Closely monitored for symptoms over 21 days
- Fed with an appropriate breast milk substitute.
- Restarted on breastfeeding after two consecutive negative tests of breast milk.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited