- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
'We Have The Means To Prevent 80% Heart Attacks And Strokes', Expert Urges NHS To Give 'Polypill'

Image Credits: Canva
Heart attacks and strokes are among the leading causes of death globally, with millions suffering from cardiovascular diseases (CVD) every year. There are more than seven million people in the UK alone, with about 100,000 patients experiencing heart attacks annually. However, a group of researchers at University College London (UCL) estimate that one 'polypill' taken daily day could eliminate a majority of these cases dramatically lowering death tolls.
The proposed polypill, a combination of a statin and three blood pressure-lowering drugs, has been under study for over two decades. Experts argue that introducing this pill universally for individuals aged 50 and above could be more effective than the current NHS Health Check, which assesses risk factors every five years for those aged between 40 and 74.
Studies have repeatedly proven the effectiveness of the polypill in preventing CVD. A groundbreaking 2019 study in The Lancet found that five years' use of the polypill cut the risk of heart attack and stroke by a third. In addition, previous modelling analyses have estimated that if given universally to people over 55, the polypill might be able to prevent 80% of heart attacks and strokes.
Today, the NHS Health Check follows a risk-based model in which patients are tested for CVD risk factors and treated with drugs accordingly. Yet, as per UCL's study, this system has serious flaws:
Low Uptake: Just 40% of those eligible for the NHS Health Check choose to have it, leaving a considerable number of at-risk patients undiagnosed and untreated.
Ineffective Prediction of Risk: The majority of heart attacks and strokes happen to people at average risk levels, thus making it challenging to identify the need for intervention effectively.
Limited Effectiveness: Even at maximum take-up, the NHS Health Check programme is predicted to have fewer health impacts compared to a polypill initiative applied to the whole population.
Simplicity and Affordability of the Polypill Strategy
One of the big benefits of the polypill is that it is so easy. In contrast to the existing screening-based model, the polypill scheme would not involve complicated medical tests or lengthy risk assessments. Instead, people reaching 50 would just have to fill out a few questions to determine possible side effects before they were prescribed.
Professor Aroon Hingorani of the UCL Institute of Cardiovascular Science, one of the strongest proponents of this scheme, says:
"Finally, the time is now to do much better on prevention. A population approach would prevent a lot more heart attacks and strokes than is done today with a strategy of trying to target a smaller group only."
Aside from the possible health implications, the polypill is also an economic solution. The drugs used are off-patent, thus cheap to produce and distribute. With the vast economic cost of managing CVD-related illnesses, a preventive model could result in substantial cost-saving for the NHS in the future.
The polypill has been proven to be effective by numerous international trials. In 2019, a randomised trial in rural Iran discovered that participants who took the polypill for five years had a 34% reduced risk of having a heart attack or stroke compared to non-participants.
Likewise, modelling research has indicated that even if only 8% of people aged over 50 took up the polypill regimen, it would still be more beneficial to their health than the NHS Health Check programme.
Is This a Case of Over-Medicalisation?
One of the main objections to the polypill strategy is the suggestion that it might result in the unnecessary medicalisation of a significant proportion of the population. But, it is argued, it should be considered as a preventative measure, not as mass medication.
Professor Sir Nicholas Wald of UCL's Institute of Health Informatics explains:
"Instead of being a 'medicalisation' of a significant proportion of the population, a polypill programme is a prevention measure to prevent an individual from becoming a patient."
He compares it with public health measures like water fluoridation or compulsory seatbelts—interventions that have been shown to have a significant impact in reducing public health danger at low individual cost.
With the evidence in favour of the polypill's effectiveness and viability overwhelming, experts are calling on the NHS to act now. It is their belief that substituting the NHS Health Check with a polypill-based prevention program could be the UK government's flagship policy under its pledge to put disease prevention ahead of cure.
As Professor Hingorani points out, "The status quo is not a justifiable option." With CVD still a major cause of death globally, taking a population-wide polypill approach could be a turning point for preventative medicine, potentially saving thousands of lives annually. The question now is whether the NHS will take up this call and establish a policy with the potential to transform the prevention of cardiovascular disease on a national level.
US FDA Approves Drug To Treat Rare Childhood Syndrome
Credit: Wikimedia Commons
The US Food and Drug Administration (FDA) has approved a drug therapy to address neurologic symptoms of a rare genetic disorder — Hunter syndrome.
The X-chromosome-linked disease, occurring predominantly in males, has an estimated 2,000 affected individuals worldwide.
The drug Avlayah, developed by pharma company Denali Therapeutics, targets certain individuals with Hunter syndrome (Mucopolysaccharidosis type II or MPS II).
It is the first therapy to address the neurologic complications of Hunter Syndrome, such as
- progressive cognitive decline,
- behavioral problems,
- hydrocephalus,
- spinal cord compression,
- seizures,
- carpal tunnel syndrome.
“Today is a milestone day for children and their families battling Hunter syndrome,” said FDA Commissioner Marty Makary, in a statement.
“Avlayah is the first product approved to address neurologic complications of Hunter Syndrome, a very rare and often severe X-linked disorder in children, affecting about 500 people in the US, almost exclusively males,” added Acting CDER Director Dr. Tracy Beth Hoeg.
The FDA noted that Avlayah, the once-weekly drug given via IV infusion, must begin in presymptomatic or symptomatic pediatric patients weighing at least 5 kg before advanced neurologic impairment.
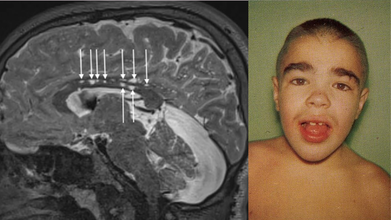
What Is Hunter Syndrome?
Hunter syndrome is a rare inherited lysosomal disorder in which sugar molecules called glycosaminoglycans build up within the cells’ lysosomes.
The condition affects physical and mental development and causes abnormalities in the skeleton, heart, respiratory system, brain, and other organs.
Hunter syndrome is a rare congenital metabolic disease. It was first reported in 1917 by a Canadian physician, Charles Hunter, in two brothers in a family.
The brothers presented typical signs, such as
- short stature,
- inguinal hernia,
- macroglossia,
- enlarged skull,
- decreased hearing,
- coarse facial features,
- protruded abdomen with hepatosplenomegaly,
- umbilical hernia,
- skeletal deformities.
The younger brother had symptoms of Central Nervous System (CNS), including seizures and cognitive decline, while the older brother did not have CNS involvement.
The estimated incidence is 1 in 162,000 live male births.
How The FDA Approved Avlayah
The FDA approval came after Avlayah showed promise in reducing cerebrospinal fluid heparan sulfate — one of the glycosaminoglycans that accumulates in the body in this disorder and is linked to the organ damage that occurs in early childhood.
The phase 1/2 multi-cohort, single-arm, open-label trial enrolled 47 pediatric patients with Hunter syndrome aged 3 months to 13 years.
Of these, 44 patients with measurements at had a 91 percent average decrease from baseline in CSF.
Denali is now conducting a randomized clinical trial that is more than 95 percent enrolled to evaluate the clinical benefit of this product.
"In the meantime, families with young children with Hunter Syndrome will have access to a product that may favorably alter the course of the disease at the crucial time in life when there is the greatest potential for benefit," Hoeg said.
Are There Any Side Effects?
Avlayah’s labeling includes a boxed warning for allergic reactions, including anaphylaxis, associated with the drug.
The FDA recommended that patients start therapy in a health care setting with appropriate medical monitoring and support measures.
The common side effects of Avlayah include
- upper respiratory tract infection,
- ear infection,
- fever,
- anemia,
- cough,
- vomiting,
- diarrhea,
- rash,
- COVID-19,
- runny nose,
- nasal congestion,
- fall,
- headache,
- skin abrasion,
- hives.
The FDA also suggested that healthcare workers monitor
- hemoglobin levels due to the risk of anemia,
- kidney function and urine protein levels due to
- the risk of membranous nephropathy (a kidney disease).
CDSCO Launches National Crackdown On Unapproved Medicines

Credit: Canva, CDSCO
The Central Drugs Standard Control Organisation (CDSCO) has now launched a nationwide crackdown on unapproved Fixed Dose Combination (FDCs) after 90 combination medicines that were being sold without mandatory central approval were busted last week.
CDSCO, India's apex drug regulatory body in the country, made the shocking discovery after scrutinizing drug samples uploaded on the SUGAM portal, the government’s online system for drug testing data.
Several of these samples were found to fall under the ‘new drug’ category but lacked approval from the central authority. As a result, the CDSCO wrote a letter to all states and union territory drug controllers, asking them to investigate manufacturers and marketers of these FDCs.
The letter reads: "The SUGAM lab testing data for the year 2025, a large number of drug samples (FDCs) are detected as unapproved and fall under the category of 'New Drug'. No new drug shall be manufactured for sale unless it is approved by the Licensing Authority 'as defined in Rule 3 of New Drugs and Clinical Trial Rules, 2019, Further, as per Rule 80 of New Drugs & Clinical Trial Rules 2019, a person who intends to manufacture new drug in the form of API or Pharmaceuticals formulation, as the case may be, for sale or distribution, shall make an application for grant of permission to the Central Licensing Authority in Form CT-21 along with a fee as specified in Sixth Schedule."
"The presence of unapproved drugs in the supply chain is a matter of serious concern, posing potential risks to public health and safety. It also indicates non- compliance with the provisions of the Drugs and Cosmetics Act, 1940, and rules made thereunder.
"Accordingly, please initiate appropriate investigation and regulatory action against the concerned manufacturers, marketers, and other stakeholders, as deemed fit. Kindly ensure strict monitoring and enforcement to prevent manufacture, sale, and distribution of such unapproved drugs," the letter states, on appropriate action against the sale and distribution of unapproved drugs.
FDCs are drugs that contain two or more active ingredients in a single formulation. The CDSCO has asked states to investigate and submit reports on the action taken at the earliest.
What Made It To The Unapproved List Of FDCs?
Cough And Cold Medicines
Cough and cold combination medicines have formed the single largest group. At least 14 to 16 entries show combination of ingredients found in everyday pharmacy shelves: dextromethorphan, ambroxol, guaiphenesin, chlorpheniramine, phenylephrine, terbutaline, and menthol in various permutations.
Several of these are sold as flavoured syrups for children. Budesonide-levosalbutamol inhalation suspension that is used for asthma and chronic obstructive pulmonary disease, too features in the list.
Nutritional Supplements
The next group is of the vitamins, minerals and other nutritional supplement which has roughly 18 to 20 entries. They include:
- Multivitamin capsules
- Iron-folic acid syrups
- Calcium-vitamin D3-K2 combinations
- Abapentin-methylcobalamin preparation
This group has accounted for at least 10 entries, which include antifungal creams that could lead to potential misuse and skin damage when sold without prescriptions.
Anti-Diabetic Medicines
This has accounted for six entries, and the combination includes:
- Glimepiride paired with metformin or pioglitazone
What Is India's Rule For FDCs?
Under India's New Drugs and Clinical Trial Rules of 2019, any FDC is treated as a new drug and must have the central government's approval before it could be manufactured and sold. The regulator's letter noted that there were presence of unapproved drugs in the supply chain that could pose risks to public health. This also amounts to a violation of the Drugs and Cosmetics Act, 1940.
“The presence of unapproved drugs in the supply chain is a matter of serious concern, posing potential risks to public health and safety. It also indicates non- compliance with the provisions of the Drugs and Cosmetics Act, 1940, and Rules made thereunder," it said.
DCGI urged states and UTs "to examine the unapproved FDCs in generic name as mentioned in the attached annexure". This is done to check whether any approval has been granted by the local office. "Accordingly, please initiate appropriate investigation and regulatory action against the concerned manufacturers, marketers, and other stakeholders, as deemed fit. Kindly ensure strict monitoring and enforcement to prevent the manufacture, sale, and distribution of such unapproved drugs," the letter noted.
‘Breakbone Fever’: US CDC Warns Of Dengue Surge Across 17 Countries

Credit: Canva
Breakbone Fever, also known as dengue, is a mosquito-borne disease that is once again on the rise, with the U.S. Centers for Disease Control and Prevention issuing a travel alert across 17 Countries.
The federal agency flagged 'Level 1' risk for breakbone fever, calling for practicing usual precautions. It stated a higher-than-expected number of cases and urged people planning to travel to countries with an uptick in cases to be aware of the risk.
The CDC alert issued on March 23 identified 17 countries reporting an increased number of cases of dengue. These include: Afghanistan, Bangladesh, Bolivia, Colombia, Cook Islands, Cuba, Guyana, Maldives, Mali, Mauritania, New Caledonia, Pakistan, Samoa, Sudan, Timor-Leste, Vietnam, and the United States territories of American Samoa, Puerto Rico, and the US Virgin Islands, where local transmission is already common.
In 2026, the US reported a total of 496 dengue cases to date, and the vast majority of these cases were reported among people who contracted the illness while traveling abroad.
The CDC advised travelers to risk areas to prevent mosquito bites by
- using an EPA-registered insect repellent,
- wearing long-sleeved shirts
- long pants when outdoors,
- sleeping in an air-conditioned room or a room with window screens.
What Is Dengue? Why Is It Called Breakbone Fever
Dengue is a disease caused by a virus spread through mosquito bites. It is transmitted through infected mosquitoes, primarily the species Aedes aegypti.
The breakbone fever is caused by an infection with any of four different dengue viruses. These include:
- Dengue virus type 1 (DENV-1 or DEN-1)
- Dengue virus type 2 (DENV-2 or DEN-2)
- Dengue virus type 3 (DENV-3 or DEN-3)
- Dengue virus type 4 (DENV-4 or DEN-4)
Common Symptoms of the dengue are:
- Sudden onset of high-grade fever.
- Intense headache
- Severe muscle, joint, or bone pain.
- Skin Rash that often appears 2–5 days after the fever starts
- Nausea and Vomiting
- Minor bleeding
- Fatigue.
The disease can take up to 2 weeks to develop, with illness generally lasting less than a week.
However, it can quickly become severe within a few hours, usually requiring hospitalization.
In severe cases, health effects can include hemorrhage (uncontrolled bleeding), shock (seriously low blood pressure), organ failure, and death.
Breakbone Fever: Global Burden
According to the World Health Organization (WHO), about half of the world's population is now at risk of dengue.
It estimates that:
- About 390 million dengue infections occur annually worldwide
- Nearly 100 million people develop symptoms each year
The two main authorized vaccines in the world against dengue are Dengvaxia and Qdenga.
These vaccines are designed to protect against all four serotypes of the virus, with a focus on reducing severe disease and hospitalizations.
In addition, the Butantan-DV vaccine developed by the Butantan Institute in São Paulo has shown potential to be over 80 percent effective in preventing the risk of severe disease for up to five years. It also offers broader protection against all four dengue serotypes.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited