- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
World Ovarian Cancer Day 2025: Theme, Significance, and History

Credits: Canva
Observed each year on May 8, since 2013 is the World Ovarian Cancer Day which is an initiative of the World Ovarian Cancer Coalition. The day unites global efforts to raise awareness about this 'silent' and deadly disease. It also emphasizes the importance of recognizing the subtle symptoms and advocates for early diagnosis.
History of World Cancer Day
The first World Ovarian Cancer Day was launched by Target Ovarian Cancer- a charity organization in the year 2013. It is the world's largest cancer charity organization that finds life-saving research and provides assistance to women who are undergoing treatment. Target Ovarian currently collaborates with over a hundred ovarian cancer charities in 32 countries.
Theme of World Cancer Day 2025
"No Woman Left Behind". This year's theme for World Ovarian Cancer day is "No Woman Left Behind" which will focus on advocating and drawing the attention of policymakers regarding the dissimilarity existing in ovarian cancer care from around the world.
As per the International Society of Gynecologic Cancer, ovarian cancer, based on Globocan's 2020 data, is the 7th most common cancer among women and 8th most common cause of death occur globally.
Every year, around 314,000 women are diagnosed, while 207,000 die from the disease. It is more prevalent and is predicted to be on 40% rise by 2040 in low resource countries bearing the greatest burden 70% of women diagnosed each year.
As per the 2018 Every Woman Study, it was found that many women are being left behind as they wait for diagnosis, this is why this year's theme is called "No Woman Left Behind."
The goal also helps to educate about ovarian cancer globally, especially in underdeveloped or low-income countries. It can also work as a call to bring all global leaders to a single platform to invest in ovarian cancer research and development.
Furthermore, it helps in promoting and enabling the reach of effective screening and treatment for ovarian cancer to prevent any further complications.
Lastly, it helps in educating and empowering every woman about their own ovarian health and, in case of any warning symptoms, seeking medical attention.
What Are The Common Symptoms of Ovarian Cancer?
While early stage ovarian cancer could be asymptomatic, women are more prone to experience these symptoms, if the illness has progressed:
- Abdominal pain
- Bloating
- Sudden urge to urinate
What Exactly Is Ovarian Cancer?
As per the Centers for Disease Control and Prevention (CDC), ovarian cancer is a group of diseases that originates in the ovaries, or in the related areas of the fallopian tubes and the peritoneum.
Women have two ovaries, located on either side of the uterus in the pelvic region. These ovaries produce female hormones and release eggs needed for reproduction. Connected to the uterus are two fallopian tubes—thin, elongated structures that extend from each ovary. The eggs travel from the ovaries through these tubes to reach the uterus.
Ovarian cancer includes several types of tumors and subtypes. The most common type is adenocarcinoma, with serous adenocarcinoma being the most frequent subtype. Most serous adenocarcinomas are high-grade, meaning they grow and spread quickly.
“Papa, I Can’t Bear the Pain”, Says Indian-Origin Man Who Dies After Eight-Hour ER Wait in Canada

"Papa, I'm in pain," said the 44-year-old Indian origin man, Prashant Sreekumar to his father, before he died at a Canadian hospital's ER due to delay. He had a cardiac arrest and was rushed to the Grey Nuns Community Hospital in Canada's Edmonton. He had been complaining of severe chest pains at work on December 22. The 44-year-old was also father of three, and was kept in the hospital's emergency room waiting area for over eight hours. This has now sparked serious questions on Canadian healthcare system.
His father, Kumar Sreekumar told the Global News that he was checked in at triage and then seated in the waiting room. When his father reached the hospital, he told him, "Papa, I cannot bear the pain."
The father said that his son felt the pain was a '15 out of 10'. The staff had given him some Tylenol for his pain, but his blood pressure kept increasing.
"It went up, up, and up. To me, it was through the roof," his father said. He was finally called for treatment after more than eight hours of wait."After sitting maybe 10 seconds, he looked at me, he got up and put his hand on his chest and just crashed," his father said.
Nurses raised the alarm and attempted to revive him, but their efforts were unsuccessful. Prashant Sreekumar died from what is believed to be a cardiac arrest. He is survived by his wife and three children, aged three, 10 and 14.
Grey Nuns Hospital, which is part of the Covenant Health network, said it could not comment on individual patient care. In a statement to Global News, the organization confirmed the death is being reviewed by the Office of the Chief Medical Examiner.
“Our thoughts are with the patient’s family and friends. The safety and care of our patients and staff remain our highest priority,” the statement said.
External Affairs Ministry spokesperson Randhir Jaiswal in New Delhi, said that the person who died was a Canadian citizen and the government must look into the matter. “The person is of Indian origin but he happens to be, I understand, a Canadian national. So the Canadian government should take responsibility in the matter,” he said at a media briefing.
What Is A Cardiac Arrest?
As per the Heart Organization, a cardiac arrest is the abrupt loss of heart function in a person who may or may not have been diagnosed with heart disease. It happens because of an electrical issue that makes your heart stop beating. Your heart stops pumping blood and you become unconscious.
Symptoms Of Cardiac Arrest
- Fatigue
- Dizziness
- Shortness of breath
- Nausea
- Chest pain
- Heart palpitations (fast or pounding heart beat)
- Loss of consciousness
Who Are At More Risk Of A Cardiac Arrest?
If you follow a lifestyle heavily indulged in alcohol or drug abuse, or have a family history of heart disease or cardiac arrest, or have a heart disease, high blood pressure, high cholesterol, low potassium or magnesium, obesity or indulge into smoking, you make be more prone to having a cardiac arrest.
The phrases “heart attack” and “cardiac arrest” are often used as if they mean the same thing, but they refer to two distinct heart conditions.
A heart attack happens when a blockage in one or more arteries cuts off blood flow to the heart. This lack of blood and oxygen damages the heart muscle. A heart attack can raise the risk of cardiac arrest because it may disrupt the heart’s electrical signals. When cardiac arrest strikes suddenly in someone without known heart disease, it is often triggered by a heart attack.
Australia Issues Advisory Warning Travelers Of Counterfeit Rabies Vaccines Found In India
Credits: Canva and Australian Government, Department of Health, Disability and Ageing
Australia issued a health advisory warning travellers and healthcare providers about counterfeit batches of a rabies vaccine that have reportedly been circulating in India since November 1, 2023. The alert has raised concerns for anyone who may have received the vaccine while travelling or living in the country.
This Is What The Australian Advisory Says:
The warning was issued on December 22 by the Australian Technical Advisory Group on Immunisation. It flagged counterfeit batches of the rabies vaccine Abhayrab. While the vaccine is not supplied or used in Australia, the advisory notes that Australians or other travellers who were vaccinated in India could still be at risk.
The advisory clearly states that people who may have received the counterfeit vaccine might not be fully protected against rabies. As a precaution, it recommends that they receive replacement doses using a rabies vaccine that is registered and approved for use in Australia.
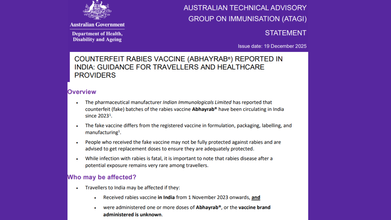
As it can be difficult to verify whether a dose was genuine or fake, the advisory takes a cautious approach. It says that anyone who received Abhayrab in India on or after November 1, 2023, should be considered as potentially having been given a counterfeit vaccine. Such individuals should be offered replacement doses as per Australian guidelines.
Why rabies protection is critical
Rabies is a viral zoonotic disease that attacks the central nervous system. In humans, it is most commonly transmitted through the bite of an infected dog. According to the World Health Organization (WHO), once rabies reaches the central nervous system and symptoms begin to appear, the disease is fatal in almost all cases.
India continues to bear a significant burden of the disease. WHO estimates suggest that rabies causes between 18,000 and 20,000 deaths every year in the country. India alone accounts for about 36 percent of rabies deaths globally, making effective vaccination and timely treatment especially critical.
Vaccine manufacturer responds
Abhayrab is manufactured by the Human Biologicals Institute, which is a division of Hyderabad-based Indian Immunologicals Limited. Responding to the advisory, the company said that it had proactively identified an issue in January related to a specific batch of the vaccine, as reported by Scroll.
According to the company, the issue involved Batch Number KA 24014, which was found in the marketplace with packaging that differed from the original. Indian Immunologicals Limited said it immediately informed Indian regulators and has been working closely with regulatory authorities and law enforcement agencies to address the issue. A formal complaint has also been lodged to support an investigation.
The company stressed that every batch of vaccine it produces is tested and released by the Central Drugs Laboratory under the Government of India before being made available for public use.
Broader concerns around medical quality
The advisory also comes at a time when India-made medical products have faced scrutiny abroad. In recent years, deaths allegedly linked to Indian-manufactured cough syrups were reported in countries like Gambia and Uzbekistan. Separately, Indian-made eye drops were suspected to be linked to infections in Sri Lanka.
Read: After Coldrif, WHO Bans 2 More Drugs, But This Is Not the Only Death from Indian Cough Syrup
Indian Immunologicals Limited, however, reiterated its commitment to safety and quality. It noted that Abhayrab has been manufactured since 2000, with over 210 million doses supplied in India and more than 40 countries. The company said the vaccine holds nearly 40 percent of the market share and assured healthcare professionals and the public that supplies made through authorized distributors are safe and meet quality standards.
Stranger Things Star Millie Bobby Brown Lives With Unilateral Deafness: Here’s What The Condition Means

Credits: Canva/AP
Millie Bobby Brown has built an impressive career, all while quietly managing a few health concerns along the way. From becoming a household name through Netflix’s hugely popular Stranger Things to leading films like Enola Holmes, the Gen Z actor (now a married mother of one) has made a strong mark in Hollywood. What many people may not realise is that her work has, at times, been shaped by a hearing-related condition. Brown has lived with hearing loss for most of her life, a fact that often goes unnoticed.
Millie Bobby Brown Reveals Having Unilateral Deafness
Brown first spoke publicly about her hearing condition in a 2017 interview with Variety, where she shared that she has had hearing loss in one ear since birth. Even early in her career, she was clear that she would not allow it to stand in the way of her passion for performing. “I just started to sing, and if I sound bad I don’t care, because I’m just doing what I love,” she said at the time. “You don’t have to be good at singing. You don’t have to be good at dancing or acting. If you enjoy it and it makes you happy, you should do it.”
While Brown rarely focuses on her hearing loss, she has spoken about how it affects her daily life. In a conversation with Call Her Daddy host Alex Cooper, she explained that certain sounds, like loud chewing, do not bother her because she can mostly hear herself when she eats. She also shared that her husband, Jake Bongiovi, whom she married in 2022, sometimes jokes that she has “selective hearing.” In reality, she says sounds often feel “muffled, like being underwater.” Brown admitted that she does miss important moments, including hearing directors call out “action” or “cut” on set.
What Is Unilateral Deafness?
Unilateral hearing loss happens when hearing is affected in one ear while the other ear functions normally. Even with hearing in one ear, this condition can make it difficult to understand speech clearly and to identify where sounds are coming from.
The level of hearing loss in one ear can range from mild to severe. When there is little to no hearing at all in one ear, it is described as severe or profound hearing loss, also known as single-sided deafness. Unilateral hearing loss may be present at birth, develop gradually, or appear suddenly. Depending on the cause, options such as hearing aids or cochlear implants may help improve hearing, according to the Cleveland Clinic.
Unilateral Deafness: What Are The Symptoms?
Many symptoms of unilateral hearing loss are similar to those seen with hearing loss in both ears. You may:
- Ask people to repeat what they’ve said
- Increase the volume on your television, laptop, or phone
- Struggle to follow conversations, especially in noisy places like restaurants or busy workplaces
- If hearing is affected in only one ear, tinnitus, or ringing, may occur on that side alone. You may also notice that you tend to rely more on one ear when speaking on the phone or listening to others.
- Although unilateral hearing loss often develops slowly, it can also happen suddenly. If you experience a sudden loss of hearing in one ear, it’s important to seek medical advice promptly.
What Causes Unilateral Hearing Loss?
Doctors do not yet fully understand all the reasons why hearing loss occurs in just one ear. Causes can differ between adults and children. In children, hearing loss may be linked to genetics or infections. Possible causes include:
- Noise-related hearing damage
- Certain inherited conditions, such as neurofibromatosis Type 2, which can lead to acoustic neuromas in one ear
- Head injuries
- Traumatic brain injury (TBI)
Unilateral Hearing Loss: Is There Treatment Available?
According to the American Academy of Audiology, treatment depends on the underlying cause and the severity of the hearing loss. Available options may include:
- Hearing aids: These are typically worn to support sound perception when one ear is affected
- Contralateral routing of signal (CROS) devices: This setup uses two devices. One acts as a microphone on the non-hearing side and sends sound to a hearing aid worn on the functioning ear
- Cochlear implants: These may help restore hearing in the affected ear and improve speech understanding and sound awareness
- Bone-anchored hearing aids: These devices transmit sound from the non-hearing ear to the hearing ear through bone conduction
- Frequency modulation (FM) systems: FM systems use radio signals to send sound directly from a microphone to a receiver, such as a hearing aid worn on the non-hearing ear
- Follow Us :



© 2024 Bennett, Coleman & Company Limited