- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
ADHD: Debunking Common Misconceptions About ADHD

ADHD may be one of the most common mental health conditions that have come to light in recent years, with our understanding of the condition much different than it was 2 decades ago. However, a few major misunderstandings still persist and can contribute to people delaying their diagnosis and necessary treatment. Here are some of the major myths about ADHD that need to be dispelled:
Myth 1: ADHD is not a real medical disorder
There’s a substantive amount of research that has shown, through brain scans, how differently an ADHD person may think as compared to a neurotypical person. In addition to this, there are also differences in brain chemicals in this region, such as dopamine, norepinephrine and glutamate operate.
There’s also a lot of data suggesting that the genes may influence ADHD. Iit has been noticed that between identical twins, if one twin has ADHD the other is likely to have it too.
Myth 2: People with ADHD are more lazy
Often accused of being lazy, patients with ADHD are often left feeling guilty for working differently. However, this does not mean that they are less productive. People with ADHD just need a different kind of work structure to function effectively.
A more organized routine with checks and balances can help someone with ADHD train their hyperfocus towards their work and getting tasks done. It’s a myth that can be particularly harmful, since these judgements can reinforce poor self-esteem in individuals that affects their ability to initiate and sustain their focus on tasks.
Myth 3: ADHD isn’t a ‘serious’ condition
ADHD is a tough condition because it requires a lot of effort to truly portray how a neurodivergent brain functions. It isn’t life-threatening or immediate, which can lead to people underestimating its implications which is very substantive as this can seep into it affecting their overall quality of life.
Myth 4: ADHD is caused by bad parenting
In a similar vein, parents with children who are suffering from ADHD may actually share some guilt, due to the fact that many people falsely believe that bad parenting “causes” ADHD. However, this simply isn’t possible.
Parenting can play an important role in providing structure and positive growth in a child, however, it cannot induce ADHD as a condition. Even the best of parents can only help in managing the symptoms or, in some cases, the advantages of ADHD, they cannot prevent it.
Myth 5: Girls don’t get ADHD as often
As hyperactivity is one of the key symptoms of ADHD, there’s a false assumption that girls are less likely to have ADHD. This is simply due to a misunderstanding of the outward-presenting symptoms of ADHD and unfortunately, girls are often less likely to be evaluated for the condition in the first place.
The issue, however, is that girls who go with their ADHD undiagnosed may go on to develop more internal symptoms related to their mood, anxiety or antisocial tendencies which they then struggle to understand. Dispelling this myth is key towards raising awareness and helping the ADHD community get the resources they need.
Tuberculosis in 2026: Why It Still Remains India’s Silent Epidemic
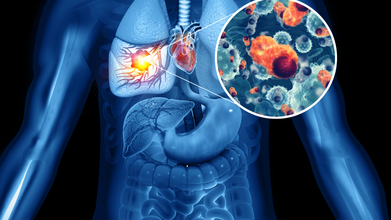
Credit: iStock
Step into a busy OPD, and you will see it: people coughing but not paying much attention. Tuberculosis is still around, just quietly spreading. By 2024, one out of every four global TB infections was recorded in India.
More than a number, each case hints at missed chances, tiny failures in spotting or stopping the disease that swell into widespread strain.
In earlier times, TB was common and very hard to recover from. Crowded homes, lack of fresh air, and low income open doors for germs to move fast. When hunger weakens people too, their bodies fail to hold back hidden sickness. But that is only part of what happens now. Conditions like smoking, drinking, high blood sugar, or HIV have slipped into view, tying daily habits closely to how often TB strikes.
After that, finding the right treatment can feel like a struggle. Some people start by visiting private clinics, shifting between different doctors until they finally learn what is wrong. Every wait means more time lost, moments when illness keeps growing without check.
Tuberculosis: What Takes The Biggest Toll?
Adults in their prime work phase feel it most. Males, particularly over the age of fifteen, carry heavier loads - a pattern the World Health Organization keeps pointing out. Yet biology alone doesn’t explain it.
Who shows up for treatment, who waits too long, who gets missed entirely, it's all written into the pattern. Older people, men, and anyone struggling with poor nutrition, using tobacco, or living with diabetes, show up more often in India’s national health data. The numbers tell a consistent story.
Tuberculosis: Late Symptoms
Here’s what happens. Tuberculosis usually shows up too late. Close to 60 percent of those feeling sick skip early help. Ongoing cough, body heat, weight loss, and night sweats are early signs. Some self-treat. For many, money becomes a barrier. Then comes the expected outcome - severe illness, tougher treatments, more time healing.
Still, false beliefs hang on. Air carries TB, not hands. Passing a meal does not pass the disease, yet shame can hold someone back from care. Cough that won’t quit, rising heat in the body, pounds slipping away, sweat at night - these hints show up early but get ignored till chances shrink.
Fighting TB in India isn’t only about medicine; it lives in habits, choices, and how people see illness. If getting help fast stays rare instead of routine, the disease keeps moving quietly through packed houses, buzzing health rooms.
Dr. Harish Bhatia is Senior Consultant in Pulmonary Medicine at Yatharth Hospital, New Delhi.
How Leg Stiffness Impacts Spine Health: Tips For Gen Z Fitness Enthusiasts

Credit: iStock
Today, the fitness scene has gained much traction among the Gen Z population. With more and more young people spending time in the gym and working out, it is important for fitness enthusiasts to remember the importance of leg stiffness and its impact on spine health. Leg stiffness has the potential to cause unnecessary strain on the spine and back during workouts.
From a neurosurgical point of view, we see that the spine is not just a mechanical support structure but a sensitive pathway through which the spinal cord and nerve roots run. Repeated micro-strain caused by poor flexibility can cause young patients to suffer early degenerative changes that may cause nerve irritation.
We also see that strengthening the abdominal muscles is essential in stabilizing the spine, thereby preventing disc injuries. Early intervention in minor complaints, such as back stiffness or nerve pain, is essential in preventing more serious problems that may need surgical intervention.
The Link Between Leg Stiffness And Spine Health
The muscles in your legs are important for your spine's health. The hamstring, hip flexor, and calf muscles are all significant players in the movement and positioning of your spine. Leg stiffness has the potential to cause unnecessary strain on the spine and back. Leg stiffness limits the movement and positioning of the hips and the spine.
When these muscle groups are tight, they alter pelvic alignment and increase load on the lumbar spine. Over time, this abnormal biomechanics can lead to disc stress and facet joint overload.
In neurosurgical practice, we often see young patients presenting with early symptoms of nerve compression where underlying muscle imbalance and stiffness play a contributory role.
Common Gym Mistakes That Increase The Risk
For young people, the main focus in the gym is on strength training, while flexibility and rest are ignored. This makes the condition of the legs stiffer. Another common error is improper posture while performing certain exercises in the gym. When the legs and hips are inflexible, proper posture is difficult, which causes pressure on the spine.
Sitting for a long time, studying, playing games on gadgets, etc., causes the hip flexors and the hamstring muscles in the legs to become stiffer, which causes pressure on the spine.
From a clinical standpoint, improper lifting techniques combined with stiffness can increase the risk of lumbar disc prolapse and nerve root irritation, conditions frequently encountered in spine clinics.
Tips to Prevent Spine Problems In The Gym
- Warm-ups: It is important to warm up the body before performing weightlifting exercises in the gym. It is recommended that the warm-up process take at least 5–10 minutes.
- Flexibility: It is important to include flexibility exercises in the gym routine, as they help in the proper movement of the legs, which in turn helps in preventing spine problems.
- Proper Posture: It is important to maintain proper posture while performing certain exercises in the gym, like squats, deadlifts, etc.
- Stretching After Workouts: This will help in the release of tension in the muscles and prevent the buildup of stiffness.
- Balance of Training and Recovery: This will help in maintaining the flexibility of the muscles and the spine.
Additionally, from a neurosurgical perspective, core strengthening plays a crucial role in stabilizing the spine and reducing the risk of disc-related injuries. Early attention to minor symptoms like back stiffness or radiating pain can prevent progression to more serious conditions requiring intervention.
Common Spine Problems To Avoid
Common spine problems to avoid during gym workouts include Herniated Disc, Sciatica, Spondylolisthesis, and Muscle Strain. These can occur from poor form, heavy lifting, or lack of warm-up.
In advanced cases, such conditions may lead to nerve compression requiring specialized evaluation and, rarely, surgical management. However, most of these issues are preventable with correct technique and conditioning.
Fitness enthusiasts in the Gen Z generation need to understand that it is very important to develop strength in the body while at the same time maintaining flexibility. The solution to the problem of a stiff leg is the foundation of protecting the spine and improving workout performance. This is achievable through the right warm-up, correct workout, and correct lifting.
Dr. Gaurav Batra is a Consultant - Neurosurgeon (Brain & Spine) at Max Hospital, Vaishali.
Meningitis Outbreak: Who Can Get The MenB Vaccine?
A recent meningitis outbreak in Kent University has led to many people wandering about the MenB vaccine and whether they should be getting it. The UK Health Security Agency (UKHSA) with NHS England and the government is already coordinating a targeted vaccination programme against Meningitis B- the strain identified to cause the outbreak.
Who Is Eligible for MenB Vaccine?
As per UKHSA, anyone in the following group has been offered preventative antibiotics which is also known as prophylaxis, is being offered the MenB vaccine. As of now, this includes:
- close contacts of those who are confirmed or suspected to have meningococcal disease
- students at the University of Kent who are normally resident on the Canterbury Campus, including those who may have now travelled home. Some staff living or working in these Halls of Residence have also been offered preventative antibiotics and are eligible for vaccination
- students who attend other universities in Canterbury, living in halls of residence or off-campus locations where there has been a case, and have been advised to take an antibiotic due to a close contact by UKHSA
- sixth form students (years 12 and 13) attending a secondary school or sixth form college in Kent where there has been a confirmed or probable case of meningococcal disease informed by local risk assessment
- anyone who visited or was working at Club Chemistry in Canterbury between 5 March and 15 March, when the venue closed voluntarily
Read: Fact Check: Did Keir Starmer Say UK ‘May Need To Go Into Lockdown’ If Meningitis Cases Keep Rising?
Is there Any Risk To The Public?
As of now, notes UKHSA that the risk of infection to the wider public remains low. This is because transmission of MenB requires close and prolonged contact to spread. This could only happen when people are living in the same household and with intimate contact such as kissing or sharing drinks or vapes.
The bacteria, notes UKHSA, are not as contagious as the other infections like measles and COVID 19.
Why Are Antibiotics Being Prescribed?
Antibiotics play an important role, and almost an immediate one when it comes to responding to an outbreak. For anyone who has been in close contact with a confirmed or suspected case, preventative antibiotics are being offered to them to clear any meningococcal bacteria they may be carrying. This will reduce the risk of them becoming ill or passing the bacteria on to others.
Most Commonly Asked Question: I've Had The MenACWY Vaccine, Do I Still Need MenB Vaccine?
The simple answer is a yes. UKHSA notes that if you are eligible for the MenB vaccine despite the fact that you have taken MenACWY vaccine, you should come forward and take the MenB vaccine. This is because the MenACWY vaccine does not protect you against the MenB strains, as they are both different strain. MenB has been identified as the primary cause of meningitis outbreak in Kent University.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited