- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Can Whooping Cough Be Deadly? Who’s at Risk and How You Can Stop It

Whooping cough, a condition once thought to be brought under control in the world today, is staging a nasty and unexpected resurgence. According to new data from the Centers for Disease Control and Prevention (CDC), the U.S. has recorded 8,077 cases of whooping cough in 2025 so far—more than double the 3,847 cases reported during the same period in 2024. This resurgence is not just a public health concern; it’s a stark reminder of what happens when vaccination rates drop and surveillance systems weaken.
Also known as pertussis, whooping cough is an extremely contagious bacterial disease that is transmitted by respiratory droplets and can happen to individuals of any age. Nevertheless, it is most dangerous to newborns and those who are not vaccinated. Sadly, just within the past six months, five children, including two infants in Louisiana, have passed away due to the complications of the illness.
The recent surge is not an isolated phenomenon. It has come on the heels of a concerning trend observed among other vaccine-preventable illnesses, such as measles. Following the COVID-19 pandemic, childhood vaccination levels plummeted. According to the CDC, in 2023–2024, a mere 92.3% of kindergartners received the complete vaccination against pertussis, compared to 94.9% in 2019–2020. Vaccine exemptions—both medical and non-medical—increased by 37% during the same time frame.
This reduction in coverage has undermined what public health professionals refer to as "herd immunity," placing vulnerable groups such as newborns and immunocompromised individuals at high risk. And because immunity from the DTaP or TDaP vaccine wanes over time, adolescents and adults can unwittingly act as carriers of the disease, transmitting it to unvaccinated infants.
Is Whooping Cough Deadly?
Yes, whooping cough can be deadly—especially for the youngest and most vulnerable. While many people recover without complications, the disease poses a serious risk for infants under six months of age. Their immune systems are still developing, and their airways are smaller, making them particularly vulnerable to severe outcomes.
According to the Mayo Clinic, complications such as pneumonia, apnea (pauses in breathing), seizures, and even brain damage can occur in infants who contract the illness. The Centers for Disease Control and Prevention (CDC) also emphasizes that babies and young children are at the highest risk of life-threatening complications, including death.
Who's Most at Risk?
Although pertussis may produce a lingering, annoying cough in adults, the outcome in infants and young children is considerably more severe. The Mayo Clinic and CDC report that babies aged less than 6 months are at greatest risk for serious complications and death. Their immature respiratory systems are more likely to be affected by pneumonia, seizures, apnea (stoppage of breathing), brain damage, and even death.
Most alarming is the reality that the illness can fail to manifest with the traditional "whoop" noise in babies. Rather, it can appear as feeding difficulty or sudden cessation of breathing—symptoms that are easily mistaken for something else until they become fatal.
Identifying the Symptoms of Whooping Cough
Whooping cough typically copies the common cold initially—sneezing, mild cough, and low-grade fever. Within one to three weeks, though, the symptoms worsen. The defining symptom is a violent, intractable cough followed by a sudden gasping breath that produces the characteristic "whooping" sound. Coughing spasms followed by vomiting are also typical.
Diagnosis is usually established through laboratory testing of throat or nasal mucus, or through blood tests to determine the presence of antibodies.
Is It Just a Bad Cough or Something More?
Pertussis is caused by the Bordetella pertussis bacteria and is highly contagious respiratory illness. The CDC believes that 80% of non-immune individuals will become infected if exposed. The bacteria bind to the cilia (microscopic hairs) of the upper respiratory tract and then release toxins that destroy the lining and lead to inflammation.
One of the major challenges is that individuals are most infectious in the initial phases of illness, usually before they even realize that they have pertussis. This makes the necessity of timely diagnosis and early isolation very crucial.
How Can You Prevent Whooping Cough?
The best protection against whooping cough is with timely vaccination. Babies are given a course of DTaP shots from two months of age, and booster shots throughout early childhood. After children are age 11, they begin to take the TDaP vaccine, which covers tetanus and diphtheria as well.
Most importantly, pregnant women should get a TDaP booster between 27 and 36 weeks of pregnancy. It enables the transfer of protective antibodies to the baby prior to birth, affording important protection during the first months of life when the infant is most susceptible.
Keep sick children at home. If your child is diagnosed with pertussis, they should remain isolated until at least five days of antibiotic treatment have been completed.
Inform and protect household contacts. Anyone living with an infected person should consult a healthcare provider about preventive antibiotic treatment.
Practice mask-wearing. If you’ve been exposed to pertussis or are awaiting test results, wearing a mask around others can help prevent further transmission.
Promote vaccine catch-ups. Parents can make sure children are up to date on all vaccinations and speak with pediatricians regarding any doses that were missed.
Educate your community. Local outreach and awareness campaigns can assist in rebuilding trust in vaccines and emphasizing the importance of community protection.
Unique Symptoms Of Vitamin D Deficiency

Credits: Canva
Long winters and lack of sunlight has renewed attention on vitamin D deficiency, a condition closely linked to bone health and overall well-being. Health data show that the problem is far more widespread than many realize, with potential consequences that range from brittle bones to mood changes.
Vitamin D and Its Role in the Body
Vitamin D plays a crucial role in helping the body absorb calcium, an essential mineral for strong bones and teeth. Without enough vitamin D, calcium absorption drops, weakening bone structure over time. This increases the risk of fractures, particularly among older adults.
Beyond bone metabolism, vitamin D also supports muscle function and contributes to a healthy immune response. Researchers have also explored its influence on mental well-being, as vitamin D receptors are present in several areas of the brain.
Deficiency Affects a Large Section of Adults
According to figures from the Robert Koch Institute, around 30 percent of adults in Germany have insufficient vitamin D levels. This is striking, given that the vitamin is produced by the body when skin is exposed to sunlight.
Experts point to modern lifestyles as a key reason. Many people spend most of their day indoors, often working in offices with little exposure to natural light. Seasonal factors also play a role, as sunlight is weaker and less frequent during autumn and winter months. In such conditions, relying on sunlight alone is often not enough to maintain healthy vitamin D levels.
Can Diet Help Fill the Gap?
Food can support vitamin D intake, although it usually provides smaller amounts compared to sunlight. Fatty fish are among the best dietary sources. Salmon, herring, eel, tuna, and pike perch contain relatively high levels of the vitamin and are often recommended for people at risk of deficiency.
Other animal-based options include eggs, liver, beef, and butter. For those who avoid animal products, plant-based sources can contribute modest amounts. Mushrooms, spinach, kale, broccoli, and Brussels sprouts are commonly mentioned. Some fruits such as avocados, kiwis, oranges, bananas, and figs are also included in vitamin D-friendly diets, though their contribution is limited.
Read: Vitamin D Supplements Under Scrutiny As It Fails Safety Test
Because many of these foods are eaten infrequently, especially fish, diet alone often fails to correct a deficiency.
Symptoms Linked to Low Vitamin D Levels
Vitamin D deficiency can show up in different ways. Many people report persistent fatigue, low mood, or depressive symptoms. While studies support a connection, researchers note that the exact biological pathways are still being studied.
Physical signs are often related to bone health. Weakened bones can increase the risk of fractures and cause general bone pain. Digestive issues and reduced tolerance to certain foods have also been reported in some cases. A deficiency is usually confirmed through a blood test ordered by a doctor.
When Too Much Becomes Harmful
While deficiency is common, excessive vitamin D intake can also pose risks. Health experts stress that overdoses do not occur through sunlight or normal diets, but through high-dose supplements taken over time.
Too much vitamin D can raise calcium levels in the blood, a condition known as hypercalcemia. This may lead to kidney damage, heart rhythm problems, and calcification of blood vessels. Individual risk varies depending on factors such as body weight, metabolism, and alcohol consumption, making medical guidance essential before supplement use.
Breast Cancer Signs That Do Not Feel Like Cancer, Explain Doctors

Credits: iStock
On World Cancer Day 2026, we at Health and Me is focussing on the most common cancer among women in India. Breast Cancer, which accounts for over 216,000 new cases every year, as per the 2022 data. This means, 28.2 per cent of female cancers are attributed to breast cancer. What is more tragic is that one woman is diagnosed with breast cancer every four minutes, and one dies every eight minutes in the country.
While, we all know that finding a lump is the red flag, there are other signs that women often miss that delays their detection. Health experts are increasingly warning that this narrow understanding may be delaying early diagnosis for many patients. New medical insights suggest that several lesser-known changes in breast tissue, skin and nipple appearance may signal cancer but often go unnoticed or get dismissed as harmless hormonal changes.
Read: More Than A Diagnosis: Cancer Survivors Share The Small Wins That Helped Them Heal
Breast Cancer Is Not Just A Lump
Data from a consumer survey commissioned by The Ohio State University Comprehensive Cancer Center shows that 93 percent of adults identify a lump as a symptom of breast cancer. But fewer than half are aware of several other warning signs that could appear much earlier.

Experts warn that this knowledge gap can be risky because not all breast cancers form lumps that are easily felt. Breast medical oncologist Ashley Pariser explains that screening mammography remains the most effective tool for detecting breast cancer at its earliest and most treatable stages. She adds that being familiar with the normal look and feel of one’s breast tissue helps people detect subtle changes faster and seek timely medical care.
Pariser notes that many breast changes can occur due to aging or childbirth. Still, she stresses that breast cancer can present in multiple ways, making it important for individuals to report unusual symptoms without delay.
Signs That Should Not Be Ignored
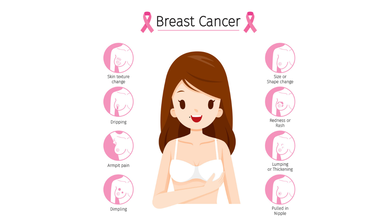
According to Dr Kanchan Kaur, Oncoplastic Breast Surgery Specialist, structural changes in the breast are among the most overlooked early warning signs. She highlights that while lumps are common indicators, deformations in breast shape such as flattening, indentation or dimpling should not be ignored.
Read: AI Detects More Breast Cancer Cases in Landmark Swedish Study
Dr Kaur also points out that an unusual increase or decrease in breast size, particularly when it affects only one breast, and sudden changes in breast symmetry may signal an underlying issue. She advises that these signs warrant clinical evaluation even if they appear painless or gradual.
Another concerning sign is skin texture change. She explains that a reddish, pitted texture resembling the surface of an orange or a marble-like area under the skin can indicate deeper tissue abnormalities. Any area of the breast that looks or feels noticeably different from surrounding tissue should be assessed by a doctor.
Nipple Changes Can Be Early Red Flags
Both research findings and clinical observations highlight nipple changes as key indicators that are often missed. Survey results from Ohio State University show that only about one-third of respondents recognized nipple inversion or retraction as a symptom of breast cancer.
Dr Kaur notes that nipples can provide early clues about breast disease. Symptoms such as newly inverted nipples, dimpling around the nipple, scaly red rashes, burning or itching, and ulceration should prompt medical attention.
Read: Oncologists Warns Of The Cancer Rising Among Women in India
Clear or bloody nipple discharge that is unrelated to pregnancy or breastfeeding is another warning sign. While discharge can occur due to benign causes, experts recommend prompt evaluation to rule out cancer.
Specialists at Moffitt Cancer Center caution that symptoms such as breast tenderness, swelling or changes in fullness are often mistaken for routine hormonal fluctuations. Because these symptoms frequently overlap with premenstrual changes, many women delay consulting a specialist.
Experts from the center advise that persistent breast pain, swelling or unusual fullness that does not resolve within a few days should be medically evaluated. They emphasize that sudden nipple inversion, discharge or skin texture changes require immediate attention.
World Cancer Day 2026: India’s 10 Most Common Cancers, Explains Doctor
Credits: Canva
Cancer trends in India are changing rapidly, driven by lifestyle patterns, environmental exposure, infections, and limited access to early healthcare in some regions. According to Dr Puneet Gupta, Chairman of Oncology Services at Asian Hospital, understanding early warning signs and adopting preventive habits can significantly improve survival outcomes.
“Cancer patterns in India are the results of multiple factors ranging from lifestyle, environmental exposure, infections and access to timely care,” Dr Gupta explained, adding that early symptoms can appear months or even years before the disease reaches advanced stages.
Breast Cancer: The Most Common Cancer In Women
Dr Gupta noted that breast cancer is frequently seen in women, especially after the age of 40. He highlighted that the disease often develops silently and without pain.
He explained that warning signs may include lumps in the breast or under the arm, changes in breast shape, skin dimpling, inward turning of the nipple, or unusual discharge. “Do not ignore these changes,” he cautioned. Regular self-examination, along with timely imaging tests such as mammography, ultrasound, or MRI, can help detect breast cancer early.
Cervical Cancer: Strongly Linked To HPV Infection
Cervical cancer mainly affects women between 30 and 60 years. Dr Gupta emphasised that HPV infection remains the leading risk factor. Early symptoms can include abnormal vaginal bleeding, bleeding after intercourse, or persistent pelvic pain, although early stages often remain symptom-free.
He stressed that routine Pap smear screening and HPV vaccination play a crucial role in prevention and early diagnosis.
Lung Cancer: Rising Risk Beyond Smoking
While lung cancer remains more common in men, Dr Gupta pointed out that cases among women are rising as well. Smoking is the primary cause, but exposure to fine particulate air pollution (PM2.5) also contributes to the risk.
He warned that persistent cough, chest pain, breathing difficulty, unexplained weight loss, or coughing blood require immediate medical evaluation, particularly in people with a history of tobacco use.
Oral Cancer: A Major Concern In India
Oral cancer remains widespread due to tobacco, gutka, areca nut consumption, and HPV infection. Dr Gupta explained that long-lasting mouth ulcers, red or white patches inside the mouth, jaw stiffness, or swallowing difficulty are early red flags. Regular dental and oral examinations can help detect early cancerous changes.
Colorectal Cancer: Lifestyle-Linked Risks
According to Dr Gupta, colorectal cancer is increasingly being diagnosed in adults around 40 years of age. Sedentary lifestyles, low-fiber diets, and excessive red meat intake are major contributing factors.
He said symptoms such as blood in stool, persistent bowel habit changes, abdominal pain, or unexplained anaemia should not be overlooked. Early screening and genetic testing in high-risk individuals can significantly improve outcomes.
Stomach Cancer: Often Shows Subtle Symptoms
Dr Gupta explained that stomach cancer may initially present as indigestion, early fullness, nausea, or unexplained weight loss. It is often associated with long-term Helicobacter pylori infection, smoking, and salt-heavy diets. Persistent digestive discomfort warrants medical attention.
Prostate Cancer: Common But Often Slow Growing
Prostate cancer typically affects men above 50 and usually progresses gradually. Dr Gupta noted that difficulty urinating and frequent nighttime urination are common early symptoms. Regular check-ups help detect the disease before complications arise.
Esophageal Cancer: Linked To Lifestyle And Nutrition
Tobacco use, alcohol consumption, poor nutrition, and iron deficiency increase the risk of esophageal cancer. Dr Gupta advised that swallowing difficulty, chest discomfort, or unexplained weight loss should prompt evaluation through tests like endoscopy or barium swallow.
Ovarian Cancer: Often Missed Due To Vague Symptoms
Dr Gupta explained that ovarian cancer frequently goes undetected due to non-specific symptoms such as bloating, abdominal discomfort, or early satiety. Women with persistent symptoms, particularly those with a family history of breast or ovarian cancer, should seek medical evaluation.
Liver Cancer: Screening Is Crucial For High-Risk Groups
Liver cancer often develops in individuals with chronic liver disease. Symptoms such as jaundice, abdominal swelling, or persistent pain usually appear late. Dr Gupta stressed that hepatitis vaccination and screening among high-risk groups are vital for prevention.
Lifestyle Changes And Screening Can Reduce Risk
Dr Gupta emphasized that although cancer cannot be completely prevented, a significant proportion of cases are linked to modifiable risk factors. Avoiding tobacco, maintaining a healthy weight, consuming balanced nutrition, managing stress, and staying physically active can lower risk.
He added that vaccinations against HPV and hepatitis further reduce cancer risk, while regular screening helps detect cancers at pre-cancer or early stages. “Education, prevention and early detection make the difference between late-stage disease and long-term survival,” Dr Gupta concluded.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited