- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Delhi Pollution Is Causing Health Issues Not Seen Before

The air quality index (AQI) has worsened in Delhi-NCR in the past few days with the Commission for Air Quality Management (CAQM) invoking stage two of the anti-pollution plan Graded Response Action Plan (GRAP). Doctors and experts have also taken note of the rise in pollution, and have observed diseases they have not seen before.
Dr Sanjay Jain, a Delhi-based ENT and a member of DocTube also noted an increase in the number of patients with respiratory issues. "I have seen a notable increase in patients with upper respiratory tract infections, chronic sinusitis, and allergic rhinitis, which are directly linked to rising pollution levels," he says. From his experience, he has noticed a rough increase of 30 to 40% of patients with pollution-related ENT issues.
What Is The Administration Doing?
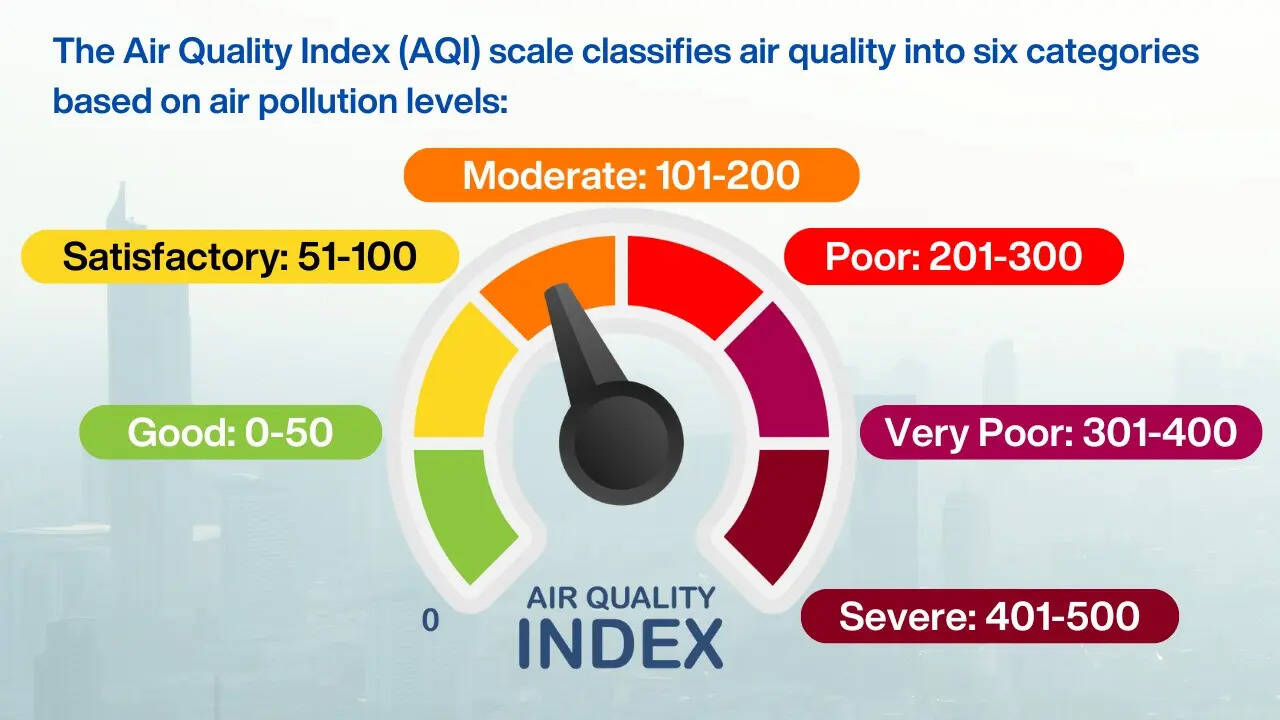
As per the System of Air Quality and Weather Forecasting and Research (SAFAR), the AQI in Delhi at 8 am today was recorded at 317, which falls under the "very poor" category. The India Meteorological Department (IMD) has predicted that the average AQI will stay in the "very poor" category in the coming days.
GRAP accounts for the restrictions on the usage of coal and firewood, and diesel generator sets in the Delhi-NCR. Furthermore, plans for mechanical sweeping and water sprinkling on the identified roads will also be carried on a daily basis. The plan expands to dust control measures at the construction and demolition sites too.
Parking fees will also be increased to discourage private transport with additional buses and metro services to start soon.
Source Of Pollution
A study titled What Is Polluting Delhi's Air? A Review from 1990 to 2022 mentions that Delhi's major contributor is road transport, while the second major factor comes from burning agricultural waste or stubble. Other factors like waste management, the construction sector, roads, and firecrackers during Diwali also lead to the increase in pollution.
Health Issues
Delhi pollution is more dangerous than we think. Not just breathing issues, but it can also lead to lung cancer and heart diseases. Studies have shown that prolonged exposure to pollution can lead to a reduction in lung function and also premature death, especially in children. It can also lead to increased risks of stroke, cognitive decline, and even pregnancy complications.
Doctors also take note of other pollution-related issues that were not seen before or are unusual. Dr Jain says that prolonged exposure to pollution can cause chronic ear infections in children due to inflammation in the Eustachian tube. "This is not commonly recognised by the people," he says. Dr Brunda MS, senior consultant, of internal medicine at Aster CMI Hospital in Bengaluru also explains that many people remain unaware of the health issues associated with pollution. Apart from shortness of breath, environmental toxins can cause brain diseases and reproductive health issues. "The subtle and slow effects of pollution often lead Understanding these relationships can help communities promote cleaner, more resilient environments," explains the doctor.
The doctor also explains the impact of pollution on the eyes as it can cause conjunctivitis or worsen any pre-existing eye infection. Dr Brunda MS also mentions that air pollution is responsible for 1.67 million deaths in India, which is 17.8% of the total deaths in the country. "There has been a 3 to 4% increase in a number of cases because of pollution," the doctor explains.
How To Stay Safe?
Dr Jain explains the precautions one can take to stay safe and prevent these diseases from happening. "Individuals can protect themselves by wearing masks, using air purifiers at home, avoiding outdoor activities during high-pollution days, and maintaining a healthy lifestyle," he explains.
The doctors also recommend wearing N95 masks, surgical masks or equivalent for effective filtration of airborne particles, consuming warm fluids and herbal teas and eating food rich in vitamin C and antioxidants that will help reduce inflammation and protect mucous membranes in the throat.
Cardiovascular Diseases Lead As India’s Top Killer: US Cardiologist Points Out Risk Factors
Credit: NYU Langone/iStock
Indians are facing an increasing burden of heart diseases, and mortality is rising faster compared to other countries. A top US cardiologist has now shared the major risk factors that range from genetics to obesity to pollution.
Cardiovascular diseases (CVDs) cause nearly 31 per cent of all deaths in India, according to the latest Sample Registration Survey (SRS) 2021-2023 data from the Registrar General of India, released in September 2025.
The SRS report highlighted cardiovascular diseases as the leading cause of death, especially among adults over 30.
Speaking exclusively to HealthandMe, Dr. Sripal Bangalore, Professor of Medicine at New York University School of Medicine, highlighted the key reasons why India is seeing a huge burden of heart diseases.
"I think it’s a combination of traditional and non-traditional risk factors. Globally, we are seeing the burden of obesity increasing, and specifically in India, genetic factors and non-traditional risk factors also play a role," Dr. Sripal said.
"There is a growing investigation into lipoprotein(a) and other causes of cardiovascular disease (in India). Obesity is a major risk factor, and I’m sure stress and pollution also add to it, with more and more data supporting these links," he added.
Data from the World Heart Federation showed that heart disease kills 28.6 lakh Indians every year. In the recent past, India has also been seeing a significantly higher rate of heart attacks and related deaths, even in children as young as 12 years old.
Also read: AHA’s New Dyslipidemia Guidelines Stress Early Screening, Lifestyle Management
What Factors Are Driving This Trend
"I think we need to know that part of it tends to be non-traditional, because in the Western world most of it is explainable by traditional risk factors like hypertension, diabetes, and hypercholesterolemia," Dr. Sripal said.
"What we see in India is that it is less about those risk factors, but more about non-traditional ones, including potentially genetic factors and lipoprotein(a)," the doctor added.
The Indian-origin interventional cardiologist also cited lifestyle factors such as stress and pollution that are significantly adding to the increased risk of cardiovascular events in the country.
AHA 2026 Cholesterol Guidelines: Relevance For India
Recently, the American Heart Association (AHA) released cholesterol guidelines, which stressed the importance of early screening, starting with teenagers.
The guidelines call for early intervention through early screening and healthy lifestyle changes, starting from childhood.
It recommends:
- Children (9-11 years): Cholesterol screening if never done before.
- Adults (30-79 years): Evaluate 10- and 30-year ASCVD risk to determine the need for early intervention
"India is a good example where LDL levels (bad cholesterol) may not be very high, like in the Western world. Many times, HDL cholesterol (good cholesterol) tends to be lower, and there are other risk factors, including lipoprotein(a), which seems to be elevated here," Dr. Sripal said.
How To Improve Heart Health
The doctor also explained whether overall diet quality matters more than just cholesterol intake.
"Diet adds to the totality of everything that we do, including increasing the risk of obesity. Cholesterol may explain some part of it, but having a heart-healthy diet is critically important," Dr. Sripal said.
The cardiologist highlighted the need to increase the intake of fruits and vegetables, as consuming natural foods is critically important.
Importantly, he also emphasized at least making sure that you have a lipid panel to check your cholesterol levels.
"We are assuming that you are staying healthy and not smoking. Checking blood pressure, it depends on your age, but at least once a year, checking your lipid panel would be critically important," Dr. Sripal told HealthandMe.
As a cardiologist, he shared that to boost heart health, the key is
- to make sure that you lead a healthy lifestyle,
- stay away from smoking,
- increase physical activity,
- reduce stress.
"Pollution is one factor, and I think we can all do our part to make sure that we don’t contribute more to environmental pollution," he noted.
Study Shows Single-use Plastics Still Rampant In India: How It Can Affect Your Health?

Credit: Toxic Link
While India’s Ministry of Environment, Forest, and Climate Change (MoEFCC) enforced a nationwide ban on identified single-use plastic (SUP) items from July 1, 2022, a new survey showed that violations continue to persist across major cities in the country, raising significant health and environmental risks.
The survey of 560 locations by Toxics Link -- an Indian environmental research and advocacy organization -- showed that 84 percent of sites across Delhi, Mumbai, Guwahati, and Bhubaneswar still use or sell banned plastic items.
Bhubaneswar recorded the highest availability of banned SUPs at 89 percent of survey locations, followed by Delhi at 86 percent, Mumbai at 85 percent, and Guwahati at 76 percent.
The survey noted that high use among street food vendors, juice shops, coconut water sellers, vegetable vendors, and ice cream parlours.
"The continued presence of banned plastic items in a majority of locations suggests that enforcement remains inconsistent,” said Ravi Agarwal, Director of Toxics Link.
“Unless implementation improves and the supply of these products is controlled, the ban will not effectively address plastic littering and pollution,” he added.
How Plastics Can Harm Your Body
Plastic carry bags, disposable plastic cutlery, cups, plates, and straws often contain chemicals like BPA and phthalates, which can interfere with the body’s hormonal balance.
BPA is an industrial chemical used to make certain plastics and resins, and its exposure has been linked to several health conditions, including an increased risk of high blood pressure.
Phthalates, another group of chemicals used to make plastics more flexible, have been found to disrupt the endocrine system, leading to potential health issues.
Also read: Your Kids’ Fast-fashion Clothing May Be Laced With High Levels of Toxic Lead
Studies have proven that BPA and phthalates can mimic the body’s hormones, particularly estrogen. This interference can disrupt the normal functioning of the cardiovascular system, leading to increased blood pressure.
Plastics also contain some highly toxic chemicals, such as flame retardants, per- and polyfluoroalkyl substances (PFAS), that can migrate into the environment and into human bodies.
According to a report by WWF, an average person could be ingesting approximately 5 grams of plastic every week.
Scientific studies have proven that the health effects of plastics include cancer or changing hormone activity (known as endocrine disruption), which can lead to reproductive, growth, and cognitive impairment.
Recent evidence also indicates that humans constantly inhale and ingest microplastics through contaminated seafood, including fish and shellfish.
In addition, microplastics have been found in tap water, bottled water, and even commonly consumed beverages, such as beer and salt.
How to Reduce the Disease Risks?
The UNDP urges individuals, organizations, and governments to work together to
- manage plastic waste,
- reduce plastic usage,
- transition to a more sustainable and resilient environment.
Other options include
- Opting for BPA-free and phthalate-free options
- Switching to reusable water bottles, plates, and cutlery made from glass, stainless steel, or other safe materials can significantly reduce exposure to harmful chemicals.
- Avoid exposing plastic bottles or lunch boxes to high temperatures, as heat can accelerate the leaching of chemicals into the water.
HIV No Longer Barrier To Organ Transplants, Say Delhi Doctors After Successful Kidney Surgery

Credit: Canva
While a weakened immune system and fear of complications once denied people with HIV access to organ transplants, doctors at a Delhi hospital have now challenged the idea with a successful kidney transplant surgery on a 43-year-old HIV-positive patient from Ethiopia.
According to the team of doctors from the Max Super Speciality Hospital, Patparganj, who successfully performed the complex living donor kidney transplant, advancements in antiretroviral therapy and transplant protocols have made such procedures increasingly safe in carefully selected cases.
“HIV is no longer a barrier to organ transplantation when managed appropriately,” said Dr. Ravi Kumar Singh, Senior Consultant, Nephrology and Transplant Physician at Max Hospital, Patparganj.
“With strict selection criteria and coordinated multidisciplinary care, patients with well-controlled HIV can achieve outcomes comparable to the general transplant population.”
Also read: India Identifies 219 Districts As Priority For Intensified HIV/AIDS Interventions
Kidney Transplant In HIV Positive Patient
The patient, who had been living with HIV for 10 years, developed end-stage renal disease 3 years ago and has been dependent on regular dialysis since then.
Before the surgery, the patient underwent extensive evaluation to ensure optimal control of HIV, including a stable immune profile and undetectable viral load.
The patient’s 33-year-old wife donated one of her kidneys. Compatibility testing confirmed matching blood groups and a negative cross-match, enabling the team to proceed with the transplant.
“Kidney transplantation in patients with HIV requires a highly meticulous and coordinated approach, given the complexities of balancing immunosuppression with ongoing antiretroviral therapy,” said Dr. Paresh Jain, Senior Director, Urology, Robotic Surgery & Renal Transplant.
“In this case, careful pre-transplant evaluation, precise surgical execution, and close post-operative monitoring were critical to ensuring a successful outcome. This procedure reflects how advances in transplant science and surgical expertise are enabling us to safely expand access to life-saving transplants for patients who were once considered high-risk,” he added.
Following the transplant, the patient has shown encouraging recovery, has been taken off dialysis, and is gradually returning to normal daily activities, the doctors said. The patient also continues on a carefully monitored regimen of immunosuppressive and antiretroviral therapy, they added.
Also read: India's Silent Crisis: Why We Must Embrace Deceased Donor Organ Transplantation
Can People With HIV Get A Transplant?
With advancements in antiretroviral therapy (ART), enabling people to live longer, HIV has now become a chronic, manageable condition. However, the HIV positive patients are now more likely to die from end-stage organ disease than from AIDS-related infections.
As per the US National Institutes of Health, people with HIV can successfully donate or receive transplanted organs with reasonable success rates.
However, health care providers must consider and monitor potential drug interactions, kidney and liver function, and HIV viral suppression in people with HIV receiving a transplant.
Further, the NIH advised HIV positive patients to continue taking all prescribed HIV medicines before and after transplant.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited