- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Explained: The History Of Birth Control Pills And Other Alternative

Birth Control Pills contain synthetic hormones which stop ovulation. Often causing nausea, headaches, weight gain, and loss of libido. Higher doses of these synthetic hormones of estrogen may cause blood clots too.
The Dark Side Of Birth Control Pills
Before the pills were released in the market. It underwent human trials. Women who underwent the experiment were not aware of such a trial. A Netflix documentary Sex Explained, documents that in the 1960s. the US government’s initiative to control the population in developing countries through sterilisation allowed an inhumane experiment. Women in countries like Puerto Rico were given these birth control pills. The dosage of hormones was ten times the hormones that were actually required.
While the pill worked wonders, it also caused many women to face side effects, some were life-threatening. More than 10 years later, the cases were finally brought to the US government.
American author, feminist activist and journalist Barbara Seaman also covered the case and published a report called The Doctors' Case Against The Pill. The report mentioned that women who consumed these pills underwent many side effects, including heart attacks, strokes and cancer.
An all-male panel invited men to testify for the birth-control pills. The Netflix documentary notes that women were not heard for the case, as a response they invited themselves. “I would like to know why is that the scientists and drug companies are perfectly willing to use women as guinea pigs and experiment testing the higher estrogen, low estrogen content of the pill," said one of the women.
Finally, in 1980, a lower dose of the hormonal pill was released, however, the side effects still existed.
Intrauterine Device (IUD)
As the IUD hit the market, a new kind, known as the Dalkon Shield was also released in 1971. Loretta Ross- a black woman who had the Dalkon Shield inserted shared about her experience in the Netflix documentary.
For the first few months, the IUD worked, however, she started to develop some serious infections. Being a black woman, she was subjected to prejudices. Judged for “being available,” and thus the OB/GYN concluded that it was STI, despite the negative test results.
One night, she lapsed into a coma and she found herself to be in the hospital when she opened her eyes. The Dalkon Shield was removed because it had a design flaw. Its thick string worked as a ladder for bacteria to climb into her uterus, resulting in serious infections.
While the shield was pulled out of the market in 1975, 3.3 million women had already used it by then, with 18 reported deaths.
It was also revealed that the makers knew about the design flaw six months before the release.
Male Birth Control Pills
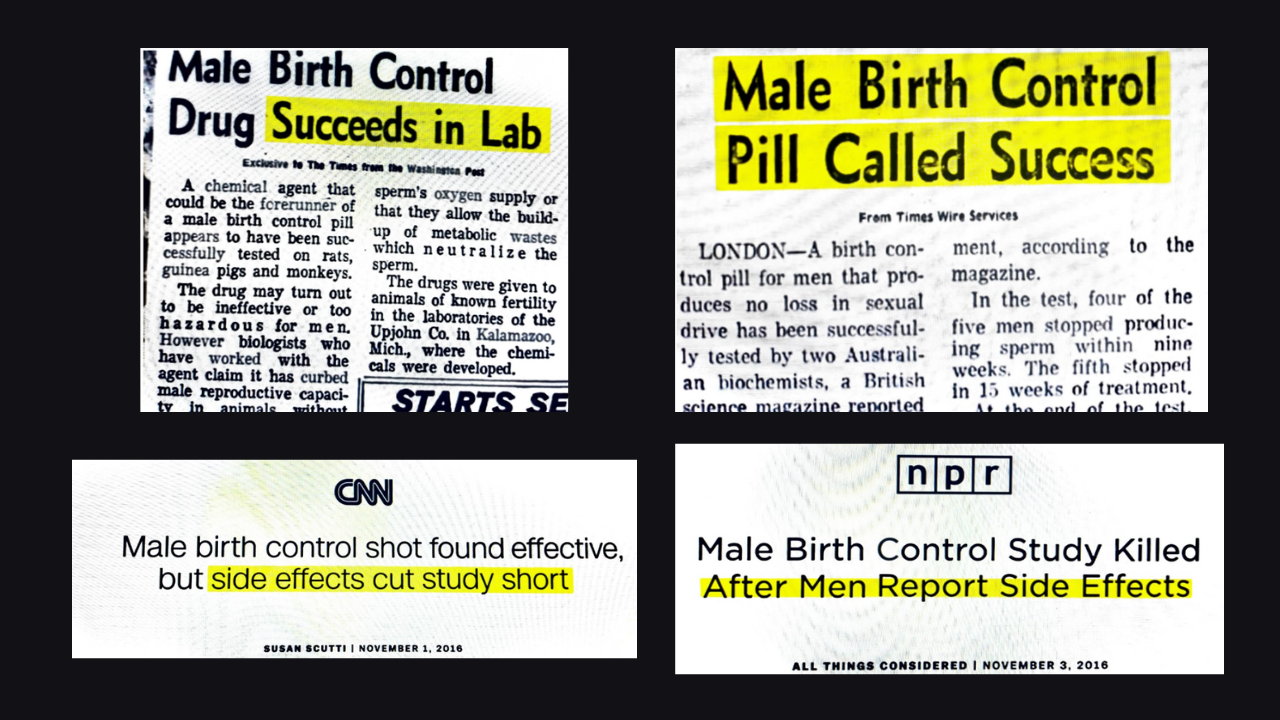
The idea of male contraception was also discussed and by 1970s, there were some promising news about it. Times Wire Services reported that a birth control pill for men was found that caused "no loss in sexual drive." It was successfully tested by two Australian biochemists. "In the test, four of the five men stopped producing sperm within nine weeks. The fifth stopped in 15 weeks of treatment," the report read.
However, as the studies went on till 2018, the pill never made it to market. In November 2016, Susan Scutti reported in CNN that the study was cut short due to the side effects of the pill. The report Male birth control shot found effective, but side effects cut the study short. Another report by NPR titled Male Birth Control Study Killed After Men Report Side Effects also seconded the claim.
While for women, those who are on birth control pills are prone to headaches, breast tenderness, acne, nausea, weight gain, irregular menstruation, mood changes, and decreased libido.
Can Botox help treat finger ulcers and gangrene?

Credit: iStock
If you think that injections of botulinum toxin -- commonly known as Botox -- are only used to make skin wrinkle-free, you may be mistaken.
A new study led by US researchers has shown that Botox injections can act as a “rescue therapy” to treat conditions such as finger ulcers, digital ischemia, and gangrene that are difficult to manage with standard therapies.
Finger ulcers (or digital ulcers) are painful open sores, while acute digital ischemia causes the fingers to become extremely painful, cold, and sometimes pale or bluish in color. Gangrene is the dangerous death of body tissue (necrosis), often turning skin black, green, or purple.
These debilitating complications, often associated with conditions like lupus, rheumatoid arthritis, systemic sclerosis, or bacterial infections, are caused by reduced blood flow to the fingers and heal poorly.
Botox injections, which work by reducing blood vessel constriction and improving circulation, may help achieve complete healing of lesions in more than 85 percent of such patients, according to a study recently published in JAMA Dermatology.
“These new findings are particularly important because therapeutic options remain limited for the cutaneous and vascular manifestations of systemic sclerosis and other autoimmune diseases,” said Dr. Netchiporouk, a scientist in the Infectious Diseases and Immunity in Global Health Program at the Research Institute of the McGill University Health Center.
Netchiporouk noted that the available vasodilator and immunosuppressive treatments are generally administered intravenously.
In contrast to Botox injections, these are also costly, minimally effective, and associated with significant adverse effects.
Also read: Botox Helped Her Burp: How Injectables Changed A 25-Year-Old's Life
The study also described the case of a 50-year-old man with a rare autoimmune disease that caused joint pain and digital necrosis (gangrene).
While traditional medications helped reduce his pain, he was forced to stop working, and the condition severely impacted his quality of life.
However, after receiving botulinum toxin injections, his pain was relieved, and sensation improved within 24 hours, and the necrosis began to improve within two weeks.
“This treatment has become an important tool, especially for patients with autoimmune vascular diseases that result in serious health consequences and for which there are few therapeutic options,” Netchiporouk said.
Also read: Why Regulatory Clarity Is Important for Safe Aesthetic Procedures in India
Botox: Safe, With Minimal Adverse Effects
The study, based on a systematic review and individual patient data meta-analysis of 30 published studies and one unpublished case involving 119 patients, found that only a few patients experienced adverse effects.
These were generally mild and short-lived, most commonly temporary muscle weakness or pain at the injection site.
“Our results show that botulinum toxin can improve blood circulation in the fingers and treat serious complications such as ulcers or gangrene, offering a safe and easy-to-administer alternative,” said Dr. Catherine Zhu, a dermatology resident at the McGill University Health Center.
Zhu added that the injections can be easily administered by rheumatologists and dermatologists in outpatient settings, reducing reliance on intravenous therapies that require hospitalization and increasing overall healthcare costs.
Importantly, in most cases, a single injection session was sufficient to achieve the desired response.
“Botulinum toxin can offer significant benefits with a favorable safety profile. It deserves further study to develop standardized protocols and optimize outcomes,” said Dr. Netchiporouk.
Can Vitamin D Deficiency Affect IVF Success Rate? Experts Weigh In

IVF offers a ray of hope to couples struggling with infertility. (Photo credit: iStock)
New Delhi: In a world where many are struggling with stress, work pressure, competition at school, and more, it does not come as a shocker that infertility has become too common. Couples often struggle to become parents, and that not only causes emotional stress but also takes a toll on relationships. But thanks to medical advancements, there are procedures like in vitro fertilisation (IVF) that make parenthood possible despite the many curveballs that infertility throws in the way. And with the precision that AI brings to the table, doctors have upped IVF success rates. But in some cases, even vitamin D deficiency can come in the way of a successful IVF treatment.
Read more: The Overlooked Role of Men in IVF: Why Their Silent Strength Is Key to Fertility Success
What is vitamin D deficiency?
Vitamin D, or the sunshine vitamin, is one of the most important nutrients that one needs for a healthy life. It influences mental health, bone and teeth strength, and, as it turns out, fertility as well. An extremely common occurrence in India, it is often seen in women of reproductive age. But can it also affect IVF success rates? Let's find out.
Dr. Kirti Singh, MBBS, MD, DNB (Obs & Gyn), Fellowship in Reproductive Medicine, Clinical Consultant, Aksigen IVF, interacted with Times Now Digital and explained how vitamin D affects women's health.
"Vitamin D is well known for maintaining calcium metabolism and bone health. Apart from that, emerging scientific evidence suggests that vitamin D may influence several pathways relevant to fertility, including ovarian function, endometrial receptivity, hormone regulation, and immune balance within the uterus. Vitamin D receptors (VDRs) are expressed in female reproductive tissues, including the ovaries, uterus, and placenta, hence having a significant impact on female fertility. Vitamin D supplementation has also been shown to have a positive effect on AMH expression. There are studies showing a positive correlation between follicular fluid (vitamin D levels) and fertilization rate. It is also known to regulate the expression of the HOXA10 gene, which helps in implantation," said Dr. Singh.

How does vitamin D deficiency affect fertility in women?
Dr. Nidhi Saluja, Centre Clinical Director, Indira IVF Hospital Limited, Gurugram, said, "Vitamin D deficiency is increasingly being recognised as an important consideration in female reproductive health, including in the context of assisted reproduction. Emerging clinical evidence suggests that low vitamin D is not merely an associated finding in infertility but a factor that may influence how ovaries function, how embryos implant, and how pregnancies progress. Since vitamin D receptors are present in reproductive tissues such as the ovaries, endometrium, and placenta, its role appears to extend beyond bone health into key aspects of fertility and reproductive support."
Read more: What Makes The IVF Journey So Hard On The Mind?
The expert went on to say that this becomes particularly relevant for women undergoing IVF, where factors such as ovarian function, embryo implantation, and endometrial receptivity are all important to treatment outcomes. Evidence suggests that women with sufficient vitamin D levels tend to show better implantation rates, improved embryo quality, and healthier endometrial receptivity. In clinical practice, low vitamin D is also often seen alongside diminished ovarian reserve and suboptimal ovarian response, especially in women already managing hormonal or metabolic challenges.
"Vitamin D status deserves greater attention as part of a comprehensive fertility assessment. While it should not be viewed as the sole determinant of IVF success, it may represent a potentially modifiable factor within broader fertility care. Identifying and addressing deficiency before conception or IVF can therefore help support a more informed and holistic treatment approach, particularly in women facing declining ovarian reserve or complex endocrine profiles," Dr. Saluja added.
What are the best sources of vitamin D?
Our main source of vitamin D, a fat-soluble steroid hormone, is sunlight. Only a small amount is obtained from our diet. In food, it is obtained from natural sources like eggs, fish, mushrooms, cod liver oil, green vegetables, yogurt, and milk. While vitamin D deficiency alone may not be the sole determinant of IVF success, studies increasingly indicate that correcting metabolic and nutritional imbalances can contribute to a healthier reproductive environment.
ICMR's Advanced Blood Test to Predict Risk of TB 1.5 Years Before Symptoms Appear
Credit: iStock
Even after being preventable and curable, tuberculosis (TB) retains its status as one of the deadliest infectious diseases more than 140 years after Robert Koch announced the discovery of Mycobacterium tuberculosis (Mtb) on March 24, 1882.
A major challenge is that millions of people carry it without knowing, and current tests often miss it. This is known as latent TB infection, where bacteria exist in an inactive state in the body.
While you do not feel sick, the infection can progress to active, contagious TB disease.
Ahead of World Tuberculosis Day, on March 24, scientists at the Indian Council of Medical Research-National Institute for Research in Tuberculosis (NIRT) in Chennai, reported developing an advanced blood test that can find TB even when it's hiding, and before it gets serious.
In the study, published in the Lancet journal eBioMedicine, the researchers explained about detecting circulating cell-free Mtb DNA in the plasma of individuals at high risk of developing TB disease via a dual target-based digital droplet PCR (ddPCR) assay.
The test was targeted at adults without a clear diagnosis of TB (asymptomatic or clinically diagnosed TB).
Using the test, the team led by Luke Elizabeth Hanna from NIRT's Department of Virology and Biotechnology, found TB in the blood up to 18 months before a person was diagnosed.
They identified eight out of 10 people at risk - all before they fell sick with the infectious disease.
“The new test performed better than all existing standard TB tests combined. This test could change how we fight TB - by finding it early, treating it faster, and stopping it from spreading,” said the team in the paper.
Tuberculosis: Advanced Blood Test
Detection of pathogen-derived cell-free DNA (cfDNA) has been gaining much attention in recent years for the diagnosis of several clinical conditions.
cfDNA is a liquid biopsy blood test that analyzes small, non-cellular DNA fragments circulating in the bloodstream.
The team found that the advanced blood test could find tiny traces of TB in the blood - even when a person feels completely healthy.
The test works by breaking a small blood sample into thousands of tiny droplets and searching each one for TB.
The study included 46 healthy household contacts of patients with pulmonary TB who developed TB within two years of follow-up, and 92 HHCs who did not progress to TB.
Plasma was obtained and subjected to testing using a ddPCR assay targeting two Mtb-specific insertion sequences, IS6110 and IS1081.
"Our findings support the diagnostic utility of ddPCR-based detection of circulating Mtb-derived cell-free DNA in plasma of individuals at high risk for progressing to active TB several months prior to clinical diagnosis," the ICMR-NIRT researchers said.
"These findings address important unmet diagnostic needs and indicate the potential of plasma-based Mtb ccfDNA detection to contribute to improved TB case detection and progress towards the WHO End TB goals," they added.
The WHO End TB Strategy
In 2024, an estimated 10.7 million people fell ill with TB worldwide, including 5.8 million men, 3.7 million women and 1.2 million children. TB is present in all countries and age groups, according to the World Health Organization (WHO).
The WHO aims to End TB by 2035, with a 95 percent reduction in deaths and a 90 percent reduction in incidence compared to 2015.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited