- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Smurf Syndrome: Rare Condition That Turns Your Skin Blue-Gray Permanently

An unusual medical condition has caught the attention of doctors and the public. Argyria, a rare disorder caused by the accumulation of silver in the body, has left people with a permanent gray or blue-gray skin tone. Though such a transformation might seem like a scene from a science fiction movie, it is very real—and the effects are long-lasting.
In this article, we shall look at the causes, symptoms, diagnosis, and treatment of argyria. We shall also address its risks, preventive measures, and new research on the condition.
Argyria is a condition resulting from the long-term accumulation of silver in the human body, leading to the permanent discoloration of skin, eyes, and other tissues especially when exposed to sunlight. This condition results primarily from the overexposure to silver particles due to occupation or ingestion of compounds containing silver.
A case that gained much attention was that of an 84-year-old man in Hong Kong, whose ashen color complexion resulted from his exposure to silver. This man had initially been admitted to the hospital upon noticing a change in his skin color. Through further analysis, silver granules were identified within his skin tissues, blood vessels, and sweat glands. His blood tests revealed that his serum silver concentration was 40 times higher than normal, and he was diagnosed with argyria. Although he claimed to have no direct exposure to silver, the case revealed the hidden dangers of silver accumulation in the body.
How Does Silver Accumulate in the Body?
Most frequently, argyria is caused due to the ingestion and inhalation of silver or a compound containing the metal. As the silver particulates enter through the bloodstream in such cases, silver deposits in nearly all tissues- skin, liver, kidneys, lungs, spleen, or even the brain.
The commonest symptom presenting in argyria is, of course when silver accumulates in the skin. Light-exposure to silver triggers a form of photoreduction with the ultraviolet components of sunlight to take on a tinge of bluish or even grayish skin. This has also been implicated in other sites, including those in the fingernails and gums, plus the eyes of some patients who develop this. Internal organs sometimes take on blueish tinges, such as the liver or spleen but only through X-rays or another medical imaging modalities.
Who Is Likely to Get Argyria?
Argyria is currently an infrequent disease, though historically, the prevalence was more pronounced. This is mainly because during the 19th century, most people had intensive exposure to silver. Some common uses of silver during the same period were its application in various industries like mining and processing and as medication. The present leading causes of argyria include:
Ingestion of Colloidal Silver
Colloidal silver is a liquid solution that has tiny particles of silver, which is mostly sold as a dietary supplement. Those who ingest colloidal silver for purported health benefits—used allegedly to boost the immune system to treat everything from diabetes and cancer—risk argyria. The use of colloidal silver has not been supported by scientific research; experts in health also warn consumers from using such.
Work Exposure
People working in silver-related industries like silver mining, manufacturing, or jewelry making. If the workers have an extended exposure to silver particles suspended in the air or deposited on the skin.
Prolonged use of medication that contains silver compounds as a component. An example of such medication is eyedrops or nasal sprays. Silver accumulation in the body may occur with a prolonged duration of medication use.
Genetic predisposition
Some rare genetic factors may predispose a few people to the condition.
Also Read: Meet Kyle Gordy Who Has Fathered 100 Babies: Here Are Surprising Health Benefits Of Sperm Donation
Symptoms of Argyria
The main symptom of argyria is the gradual appearance of bluish-gray or grayish discoloration of the skin, mainly in areas exposed to sunlight. The color change is permanent and may cause psychological distress in most patients. Other symptoms of argyria include:
- As silver builds up in the body, fingernails may darken.
- Dark spots may appear on the skin, especially in skin areas that receive regular exposure to sunlight.
- The whites of the eyes (sclera) turn a bluish-gray color.
- In some cases, argyria patients may report mild symptoms including stomach discomfort, fatigue, or headaches.
- Over time, internal organ damage such as the liver, spleen, and kidneys may occur due to silver buildup; however, these symptoms are not always observable.
The condition is not fatal, but the symptoms may be uncomfortable, and the discoloration is permanent.
How is Argyria Diagnosed?
Argyria is usually established by a case history, medical examination, and laboratory tests. A crucial diagnostic method is to undertake a biopsy on the affected areas of the skin, which, in turn can show silver particles in the tissue. Blood examination can also tell the concentration level of silver inside the blood of the patient after the diagnosis. After establishing this diagnosis, another step is toward the cause or reason behind deposition of silver.
Treatment and Management
Currently, there is no treatment for argyria. The coloration due to the condition is irreversible. However, there are several measures to help manage the appearance of the condition:
- Regular application of sunscreen can prevent the coloration from worsening since exposure to UV rays accelerates the photoreduction process.
- Though not universally successful, some patients have undergone laser therapy to minimize the appearance of the coloration, though success varies.
- Many individuals use makeup to cover the grayish tint of their skin and restore a more natural appearance.
- Some topical treatments, such as 5% hydroquinone, may help lighten the skin and reduce the appearance of the discoloration.
In addition to cosmetic treatments, it is essential for individuals to avoid further exposure to silver or silver-containing compounds to prevent the condition from worsening.
Is Argyria Preventable?
Preventing argyria is largely about avoiding unnecessary exposure to silver. If you are taking dietary supplements or medications that contain silver, consult with your healthcare provider to explore alternative options. People who work with silver should ensure that their workplace adheres to safety regulations, such as the Occupational Safety and Health Administration’s (OSHA) exposure limits for silver dust.
Argyria is a rare but serious condition that can have a significant impact on an individual’s appearance and well-being. Although modern exposure to silver is less common than in previous centuries, certain lifestyle choices, such as using colloidal silver as a supplement or working in silver industries, still pose a risk. Understanding the causes, symptoms, and prevention of argyria is key to minimizing its impact on health. Although it has no known cure, precautions and proper remedies can be availed to lessen the impact brought about by the condition.
Argyria an unrecognized cause of cutaneous pigmentation in Indian patients. Indian J Dermatol Venereol Leprol. 2013
ARGYRIA. JAMA Network. 1937
Argyria. The New England Journal of Medicine. 2025
Meningitis Outbreak: How to Differentiate The Symptoms From a Common Rash
Credits: Canva
Meningitis outbreak has led to authorities in the UK to urge students to get vaccines and antibiotics. Health and Me also reported on the menB vaccine that students 5,000 students in Kent University will be receiving. One of the common symptoms are rashes, however, how does one know if it is a meningitis rash?
How Do You Recognize Meningitis Rash?
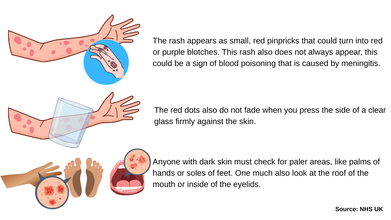
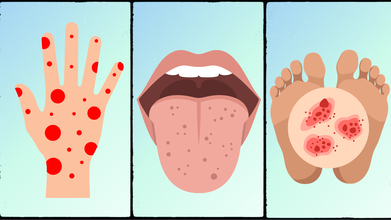
As per NHS UK, the rash appears as small, red pinpricks that could turn into red or purple blotches. This rash also does not always appear, this could be a sign of blood poisoning that is caused by meningitis.
The red dots also do not fade when you press the side of a clear glass firmly against the skin. NHS UK notes that anyone with dark skin must check for paler areas, like palms of hands or soles of feet. One much also look at the roof of the mouth or inside of the eyelids.
NHS UK notes that one must call 999, if they find such a rash.
Meningitis Outbreak UK: What Is Happening Now?
A meningitis outbreak in Kent University is now treated as a national incident, after two people have died, one of them being the student of the university. Students have been urged to get vaccines and take antibiotics as health officials are dealing with the "unprecedented" and "explosive" outbreak.
As per the UK Health Security Agency (UKHSA), 15 cases have been reported and all of them have lead to hospital admission. Cases are also expected to rise due to the incubation period of infection to when the symptoms start to appear. The incubation period is from two to 14 days.
As per experts, many of whom are affected had attended Club Chemistry in Cantebury between 5 to 7 March. UKHSA chief executive Susan Hopkins said the outbreak "looks like a super-spreader" event with "ongoing spread" through universities' halls of residence. She added: "There will have been some parties particularly around this, so there will have been lots of social mixing. I can't yet say where the initial infection came from, how it's got into this cohort, and why it's created such an explosive amount of infections."
She further said that in her 35 years working in medicine, healthcare, and hospitals, "This is the most cases I've ever seen in a single weekend with this type of infection". She added: "It is the explosive nature that is unprecedented here - the number of cases in such a short space of time." She also remarked that this was the "quickest-growing outbreak" she has ever seen in her career.
Who Should Get MenB Vaccine?
As per the University of Oxford, MenB vaccine is given to babies at 8 weeks, 16 weeks, and one year of age.
General Practitioner surgery or clinic also send an appointment for babies to have their MenB vaccination along with their other routine vaccinations.
Read: Meningitis Outbreak: What Is MenB Vaccine?
Additional doses of the vaccine are recommended for people with some long-term health conditions who are at greater risk of more severe meningococcal disease. This includes people with:
- asplenia or splenic dysfunction (a spleen that is missing or does not work properly)
- sickle cell anaemia
- coeliac disease
- complement disorders (the complement system is an important part of the immune system, and disorders of this system can increase a person’s risk to some diseases.)
Meningitis Outbreak: What Is MenB Vaccine?

Credits: Canva
Meningitis outbreak has led to death of two people, one of them being a student of Kent University. Students have also been urged to get vaccines and take antibiotics. Health and Me also reported on the outbreak and how this has led to panic among parents who are seeking for meningitis B or menB vaccine. 5,000 students in the university halls in Kent will be offered the menB vaccine in the coming days.
What Is MenB Vaccine?
London School of Hygiene & Tropical Medicine noted that over a dozen people are seriously unwell in hospital and two people have died from an outbreak of meningitis in the UK. As per the UK Health Security Agency, illness may have spread during an event attended by students in Kent. Four cases have been confirmed to be meningitis B through laboratory testing.
As per NHS UK, menB vaccine offers protection against meningococcal group B bacteria, which is identified to be the strain that has infected people. The vaccine is recommended for babies aged 8 weeks, followed by a second dose at 12 weeks and a booster at 1 year.
Read: Kent Uni Meningitis Outbreak Caused By Less-Targeted Strain B
Who Should Get MenB Vaccine?
As per the University of Oxford, MenB vaccine is given to babies at 8 weeks, 16 weeks, and one year of age.
General Practitioner surgery or clinic also send an appointment for babies to have their MenB vaccination along with their other routine vaccinations.
Additional doses of the vaccine are recommended for people with some long-term health conditions who are at greater risk of more severe meningococcal disease. This includes people with:
- asplenia or splenic dysfunction (a spleen that is missing or does not work properly)
- sickle cell anaemia
- coeliac disease
- complement disorders (the complement system is an important part of the immune system, and disorders of this system can increase a person’s risk to some diseases.)
The University of Oxford noted that from August 2025, the MenB vaccine has been offered primarily to gay, bisexual and other men who have sex with men, in a targeted programme to prevent cases of gonorrhoea. This is because these groups of people are at higher risk of acquiring gonorrhoea.
How Does Meningitis B Spread?
Neisseria meningitidis is most commonly found living in the throat. It is spread between people through close contact with secretions from the mouth or airway and usually requires close or prolonged contact between people for the bacteria to be transmitted.
Common Symptoms Of Meningitis
- Headaches
- Neck stiffness
- Fever
- Drowsiness
- Nausea or vomiting
- Increased sensitivity to light
Some meningitis infections can also cause a rash that does not disappear with pressure. However they may not be always visible in the early stages.
No Refrigeration Needed: New Vaccine May Expand Immunization Worldwide

Credits: Canva
Vaccines are among the most powerful tools in modern medicine, preventing millions of deaths each year. Yet getting those vaccines safely from laboratories to people who need them is far more complicated than many realise. Most vaccines must be kept within a strict temperature range between 2°C and 8°C from the moment they are produced until they are administered.
This temperature controlled system, known as the cold chain, depends on refrigerators, insulated transport boxes and a steady supply of electricity at every step of the journey. Any disruption can damage the vaccine and make it ineffective. Now, scientists are testing a new technology that could remove this challenge altogether.
A vaccine designed to remain stable even at room temperature has shown encouraging results in an early human trial. Researchers believe this could change how vaccines are distributed, especially in regions where refrigeration is difficult to maintain.
The Challenge Of Keeping Vaccines Cold
Vaccines are sensitive biological products. Exposure to excessive heat or freezing temperatures can damage their active ingredients and reduce their ability to trigger an immune response.
To avoid this, countries rely on a carefully managed cold chain that transports vaccines from manufacturing facilities to warehouses, regional storage centers and finally to clinics. This process requires specialised equipment, trained staff and constant monitoring of temperatures.
However, maintaining this system is both expensive and complex. Equipment failures, power outages and transport delays can disrupt the cold chain at any stage. In rural or remote regions where electricity supply is unreliable, these challenges become even more serious.
Global health experts estimate that a large number of vaccines are lost every year because of temperature control failures during storage and transport. This leads to wasted doses, increased costs and gaps in vaccination coverage.
Because of these difficulties, scientists have long been searching for ways to develop vaccines that can remain effective without strict refrigeration.
A Vaccine That Can Survive At Room Temperature
One promising development is a vaccine candidate called SPVX02, which targets tetanus and diphtheria. It has been developed by the biotechnology company Stablepharma with support from the UK Health Security Agency.
What makes this vaccine different is the technology used to stabilize its active ingredients. The formulation allows the vaccine to tolerate higher temperatures without losing potency.
Early findings from a Phase I clinical trial suggest the vaccine can remain stable at around 30°C for as long as two years. The study was carried out at the Vaccine Development and Evaluation Centre in the United Kingdom and involved healthy volunteers.
Phase I trials are the earliest stage of human testing. At this stage, researchers focus mainly on safety, possible side effects and the body’s immune response.
If further trials confirm these findings, the same stabilization technology could potentially be applied to other vaccines as well.
Why This Could Matter For India
A fridge free vaccine could have major implications for countries such as India, which runs one of the largest immunization programmes in the world.
India’s Universal Immunisation Programme delivers vaccines to millions of children every year. To reach remote villages and urban settlements, the programme depends on a vast cold chain network that includes refrigerated storage facilities, specialized transport and vaccine carriers.
Maintaining this infrastructure across a country with varied climates and uneven electricity supply can be difficult. Heat exposure during transport or power failures can lead to spoilage and wastage.
A thermostable vaccine that remains effective at room temperature could simplify this process significantly. It would reduce dependence on refrigeration, lower costs and make it easier to deliver vaccines in remote or resource limited areas.
What Happens Next
Although the early results are encouraging, the vaccine still needs to go through larger clinical trials before it can be approved for widespread use.
Future studies will involve more participants and compare the new formulation with existing refrigerated vaccines to confirm its effectiveness.
If the technology proves successful, researchers believe it could be adapted for many other vaccines in the future. That possibility could reshape how immunization programmes operate worldwide and help bring life saving vaccines to communities that have long struggled to access them.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited