- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Postpartum Nutrition Guide: Foods Every New Mom Needs For Recovery And Lactation

Becoming a mother is a life-changing experience that goes far beyond delivery. The postpartum period, sometimes referred to as the "fourth trimester," is an important time for physical recovery and emotional adjustment. Nutrition is a critical component in this period of replenishing the body, facilitating healing, and aiding lactation. A very restrictive diet might have been allowed during pregnancy. In contrast, the postpartum diet will be more accommodating of a diversity of nourishing foods that your body and your baby need to thrive.
Having carried a baby for nine months, endured the pain of labor, and labored through delivery, your body now needs to heal. Nutrition provides the basis of energy restoration, healing tissues, and support for the production of milk in breastfeeding.
As Avni Kaul, Nutritionist, Dietician, and Wellness Coach, puts it, "This time is associated with tremendous physiological changes and psychological shifts. An appropriate diet in the postpartum period helps in healing, increases milk production, and overall health."
Benefits of a Nutrient-Rich Postpartum Diet
- Speeds Recovery: Nutrient-rich foods help in tissue repair, iron replenishment, and prevention of complications like postpartum anemia.
- Helps Produce Milk: Proper hydration and nutrition help in achieving the necessary quality milk supply.
- Boosts Wellness: Balanced diet offers energy required for a new mother's challenging role.
- Overindulgence is permissible once in a while, but it is the healthier diet that would prove best for effective recovery and lactation.
Essential Nutrients for Postpartum Recovery
1. Protein: The Basis of Recovery
Protein will assist your body to rebuild and regenerate tissues of damaged parts that need repairing in cases after delivery and in making more protein for production of the milk into the baby. Top sources are: eggs, lean meats, poultry, fish, tofu, lentils, beans, and dairy products.
2. Iron: Replace your depleted reserves
Blood loss during delivery can cause a decrease in iron levels, which may lead to weakness and a weakened immune system. Iron-rich foods with vitamin C can help restore these levels and prevent anemia.
Top sources: Spinach, red meat, liver, beans, fortified cereals, and broccoli.
Vitamin C-rich foods: Citrus fruits, bell peppers, tomatoes, and strawberries.
3. Fiber: Maintaining Digestive Health
Constipation is common postpartum due to hormonal changes and reduced physical activity. Fiber-rich foods aid digestion and prevent constipation.
Top sources: Whole grains, oats, fruits, vegetables, and legumes.
4. Hydration: The Backbone of Milk Production
Lactation and hydration depend on adequate fluid intake. Target 8-10 glasses of fluids daily, including water, herbal teas, and broths. Electrolyte-rich fluids can also balance the body after delivery.
5. Vitamin B12 and Folate: Energizing and Restoring Nerve Health
B vitamins include B12 and folate. They play an important role in energy production, nerve function, and blood cell formation. These vitamins can combat postnatal fatigue and replace the blood that has been lost in delivery.
Top sources: Eggs, dairy products, beef, fish, fortified cereals, and leafy greens such as spinach and kale.
Postpartum Superfoods for Recovery and Lactation
Some foods go beyond supporting postpartum recovery and milk supply:
- Turmeric: It is the ant-inflammatory remedy in which inflammation swelling is decreased to heal well and fast.
- Fenugreek: It was historically used to augment milk.
- Oats rich in fibers with iron it keeps digestion very simple and can easily take energy with ease.
- Almond: Rich with Healthy fats and calcium almonds ensure tissue repairing.
Foods to Avoid During Postpartum
While most foods are safe, certain items should be limited or avoided for better recovery and breastfeeding outcomes:
- Caffeine: Excessive caffeine can pass into breast milk, disrupting your baby's sleep.
- Alcohol: If consuming alcohol, wait several hours before breastfeeding to ensure it doesn’t affect your milk.
- Highly Processed Foods: These are often nutrient-deficient and may contribute to fatigue.
Should New Moms Take Postpartum Vitamins?
Consult your doctor about continuing prenatal vitamins or switching to a postpartum-specific supplement. According to Avni Kaul, "Some women may need to continue prenatal vitamins while breastfeeding, while others might benefit from standard multivitamins." A healthcare provider can tailor recommendations based on your individual needs.
When Breastfeeding Twins Should You be Doubling Your Nutrition?
For mothers who nurse twins, there is an addition of around 500 calories a day per baby. Adequate hydration and the intake of calorie-rich foods is essential for each baby to thrive. Checking on wet and soiled diapers can also assure that each is being fed and hydrated correctly.
Postpartum nutrition is more than just sustenance. It fuels recovery, supports lactation, and empowers new mothers to take on the physical and emotional challenges of early motherhood. A diet rich in real, nutrient-dense foods aids in healing, replenishes energy, and strengthens the bond between mother and baby.
As Avni Kaul emphasizes, "Proper nutrition is the cornerstone of recovery, providing the strength and vitality needed during this transformative time." For personalized guidance, consulting a nutritionist or healthcare provider can help ensure your postpartum diet meets your unique needs.
Avni Kaul is a Nutritionist, Dietician and a Wellness Coach with Specialisation in Pregnancy Health and Founder of Nutri Activania in India.
Maternal Vaccination During Pregnancy Can Prevent COVID-related Hospitalization In Babies: Study

Credit: iStock/Canva
Maternal vaccination with the COVID-19 vaccine during pregnancy can be effective against severe disease and hospitalization from the SARS-CoV-2 virus in babies, according to a large study.
The study, published in the journal Pediatrics, revealed that COVID vaccination during pregnancy can protect the children against hospitalization for COVID during the first six months of life.
Also Read: COVID-19 Cicada Variant: Will It Become The Dominant Strain In The US? Know All About The Virus
Amid continuing COVID cases, babies under six months old continue to have one of the highest rates of hospitalization — one in five — due to the COVID virus in the US, as per a 2024 study.
As currently no vaccines against COVID are available for neonates and babies, the American College of Obstetricians and Gynecologists (ACOG) recommends maternal vaccination during pregnancy.
Maternal COVID Vaccination Prevented Other Infections
The retrospective study included 146,031 infants born in Norway between March 2021 and December 2023. Of these, 37, 013 (25 percent) were exposed to COVID-19 vaccination in utero.
The findings showed that babies exposed to the vaccine before birth were no more likely to visit the hospital for overall infections (of any kind) than those whose mothers did not get vaccinated in pregnancy.
However, infants whose mothers were vaccinated were about half as likely to visit the hospital specifically for COVID in their first two months of life compared to babies not exposed to the vaccine in utero.
Also Read: Olivia Munn Opens Up About Detecting No-Symptom Breast Cancer With Lifetime Risk Assessment Test
Among 3 to 5-month-old babies, the risk of a hospital visit for COVID was 24 percent lower in those exposed to the vaccine, but the vaccine's protection against COVID wore off by the time infants were older than 6 months.
Importantly, the mothers' vaccine also prevented the risk of other infections in children.
"There is often an increased risk for a subsequent infection after a viral infection, such as an increased risk of pneumonia after influenza infection, so we wanted to study whether protection against COVID-19 could influence the risk of other infections as well," said lead author Dr. Helena Niemi Eide, from the University of Oslo in Norway, the NPR reported.
"But we found that COVID vaccination in pregnancy protected the infant against COVID and had no apparent effect on other infections," Eide added.
Maternal Vaccine Recommendation in the US
Last week, the American College of Obstetricians and Gynecologists reiterated its recommendation for COVID vaccination during pregnancy.
Despite changes in federal vaccine recommendations due to the US Health Secretary Robert F. Kennedy Jr.’s anti-vaccine stance, the ACOG urged COVID vaccination for
- people who are pregnant,
- recently pregnant,
- considering pregnancy,
- lactating.
Also read: Bipolar Disorder: How Early Detection Can Help Prevent Serious Complications
"Accumulated safety data from millions of administered doses show no increased risk of adverse maternal, fetal, or neonatal outcomes associated with COVID-19 vaccination in pregnancy,” the ACOG said.
'Husband Stitch': A Medical Necessity Or Just A Tool To Objectify Women's Bodies?

Credits: AI-generated and iStock
When 36-year-old mom Angela Sanford, from Fort Mill, SC, went for an appointment for a Pap smear five years after she had her first child in 2008, her nurse midwife, who she has never seen before asked her a question she did not expect. "Who stitched you up after your first birth?"
Speaking to Healthline, Sanford shared that she just started crying when the nurse said, "This is not right." Sanford said that this was the first time she ever heard the term 'husband stitch'. Sanford was told that her stich was "too tight" by the hospitalist who managed her after her first delivery.
Also Read: US CDC Warns Of New Immune-Evasive COVID Variant In 23 Countries
“He gave you what some people call a husband stitch,” Sanford recalled the midwife telling her.
“I couldn’t connect in my mind why it would be called that. My midwife said, ‘They think that some men find it more pleasurable,’” she recalled. “My husband has been worried about me and fearful of hurting me. He would never have asked for this.”
A 'Husband Stich' - What Is It?
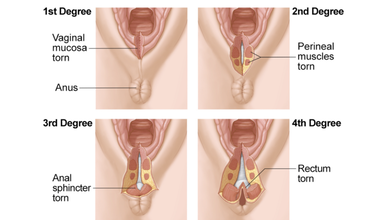
During vaginal delivery, a woman undergoes perineal tears or vaginal lacerations which means tears between the vaginal opening and anus. This causes pain, and requires stitches for grades two and higher. It also takes 4 to 6 weeks to heal. Women can experience from first to fourth degree tears.
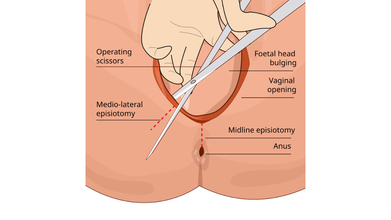
Sometimes, a surgical incision is made in the perineum during childbirth to enlarge the vaginal opening, this is called an episiotomy. However, it is not medically necessary or a routine procedure, unless it is a case of emergency.
Stiches are required in such cases that dissolves on its own. However, a 'husband stitch', also known as "daddy stitch" is an unethical practice where an extra stitch is given during the repair process that 'tightens the vagina' to increase sexual pleasure for a male partner. While it is considered a medical malpractice, it is still done to women after vaginal delivery.
Many women face difficulty after the extra stich is given to them. In Sanford's case, she felt "excruciating" pain during sex afterwards.
Read: Romanticization And The Silent Dismissal Of Women’s Pain
When Objectifying Women's Bodies Is Made A Medical Practice
Stephanie Tillman, CNM, a certified nurse midwife at the University of Illinois at Chicago and blogger at The Feminist Midwife told Healthline: “The fact that there is even a practice called the husband stitch is a perfect example of the intersection of the objectification of women’s bodies and healthcare. As much as we try to remove the sexualization of women from appropriate obstetric care, of course the patriarchy is going to find its way in there."
Harkins, 37, said that she "kind of" laughed it off when an "old, crusty Army doctor" overstitched her so she could give her husband more pleasure. In many cases, doctors do it as a routine practice without even being told by anyone. “I couldn’t even process [it], but I kind of laughed, like what else do you do when someone says that? I had just had a baby. I didn’t think much about it because the whole birth experience was so traumatizing, but now that I think about it differently, the implications of that are just crazy.”
Episiotomy Is An Excuse For 'Husband Stitch'
Dr Robert Barbieri, chair of obstetrics and gynecology and reproductive biology at Brigham and Women’s Hospital in Boston, told the Huffington Post that doctors were taught in the 50s and 60s that "routine episiotomy was good for women".
“What they thought is that if they did a routine episiotomy, they’d have a chance to repair it and that during the repair, they could actually create a better perineum than if they hadn’t done it. The idea [was] that we could ‘tighten things up,’” explains doctor.
However, a 2005 systematic review in the Journal of the American Medical Association found no benefit to routine episiotomy use. A 2017 Cochrane review “could not identify any benefits of routine episiotomy for the baby or the mother.” In 2016, the American College of Obstetricians and Gynecologists (ACOG) recommended that clinicians “prevent and manage” delivery lacerations through strategies like massage and warm compresses rather than making cuts on the perineum. Yet, this practice still continues inside the labor rooms.
Your Kids’ Fast-fashion Clothing May Be Laced With High Levels of Toxic Lead

Credit: iStock
While you may be buying fast-fashion clothes that are easy on your pocket and also give your children trendy looks, a new study highlights the risk of being laced with a highly toxic ingredient: lead.
The preliminary research, based on lab tests of several shirts from different retailers in the US, found that all the samples exceeded the country’s federal regulatory lead limits.
The US Consumer Product Safety Commission currently has a 100 parts per million (ppm) lead limit for children's products like toys and clothing.
"I started to see many articles about lead in clothing from fast fashion, and I realized not too many parents knew about the issue," said Kamila Deavers, principal investigator of the study, at Marian University in the US.
Deavers began the study after her young daughter’s lab reports showed elevated levels of lead in her blood from toy coatings.
How was study conducted?
The team tested 11 shirts that spanned the rainbow—red, pink, orange, yellow, gray, and blue. All brightly colored fabrics, particularly reds and yellows, showed higher levels of lead compared to more muted tones.
"We saw that the shirts we tested were all over the allowed limit for lead of 100 ppm," said Priscila Espinoza, from Marina.
The researchers explained that some manufacturers use lead (II) acetate as an inexpensive way to help dyes stick to the materials and produce bright, long-lasting color.
Children At Greater Risk
The researchers found the risk is particularly higher among younger kids as they tend to playfully suck or chew their clothes during play.
"Even briefly chewing these fabrics could expose children to dangerous lead levels,” they found in the study, to be presented at the forthcoming meeting of the American Chemical Society.
According to the US Environmental Protection Agency (EPA), lead exposure can lead to behavior problems, brain and central nervous system damage, as well as other negative health effects in children.
The agency considers children under six years old to be most at risk from exposure. Even low levels of lead in the blood of children can result in:
- Behavior and learning problems
- Lower IQ and Hyperactivity
- Slowed growth
- Hearing Problems
- Anemia
The researchers also pointed out safer alternatives to lead-based dyeing agents that already exist. These include natural and less harmful substances such as:
- Plant-based tannins (e.g., oak bark, pomegranate peel)
- Rosemary
- Alum.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited