- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Your DNA Could Reveal If You Had A 'Vanishing Twin' In The Womb, With A Simple Test

Image Credits: Canva
Pregnancy an extraordinary process, and for some, it begins as a twin pregnancy that they may never even know. Research says that one in eight individuals enter the world as a twin, but in a lot of these instances, one of the babies does not make it to term. Research published in the journal Human Reproduction shows that early ultrasound research indicates vanishing twin syndrome in about 12% of pregnancies. This process, referred to as vanishing twin syndrome (VTS), is when one twin fails to develop and is digested by the remaining embryo and parent. Though the deceased twin does not leave any visible impression, recent studies indicate that their existence may be traced in the DNA of the remaining sibling.
A recent study by Jenny van Dongen at VU Amsterdam in the Netherlands has revealed distinct epigenetic modifications in the DNA of identical twins. Epigenetics is a process of chemical modifications that control gene expression without changing the sequence of the DNA itself, for example, DNA methylation, in which methyl groups bind to genes to turn them on or off. For instance, during early development of the embryo, epigenetic modifications cause cells to give rise to a variety of different tissues and organs. DNA methylation, whereby methyl groups become bound to genes to essentially activate or deactivate them, is the most researched of all epigenetic modifications.
During pregnancy at an early stage, many epigenetic changes occur when the embryo coordinates different cells into a variety of the body's diverse tissues and organs. Identical twins, which develop from a single fertilized egg that eventually divides, share a unique DNA methylation pattern that differentiates them from fraternal twins and non-twins as well. The scientists found that the pattern covers 834 genes, proposing a possible way to identify whether an individual was originally part of an identical twin pair.
How DNA Can Reveal a Vanishing Twin?
The research, published in Nature Communications, compared DNA methylation data from more than 6,000 people, including identical twins, fraternal twins, and non-twin relatives. The results indicated that the epigenetic markers remain present in adulthood, so a cheek swab test might one day be able to tell whether or not a person had a missing twin.
Based on this information, researchers created a computer program that can recognize people who were once part of an identical twin set. Although the study did not test specifically if the program could detect people who had a vanishing twin, data indicate that the test could be possible in the future.
Vanishing twin syndrome happens in about 12% of pregnancies, though less than 2% of twin pregnancies give birth to both twins. The cause of VTS is multifaceted and not yet fully understood, as shown in research published in the International Journal of Fertility and Sterility.
Chromosomal abnormalities or genetic mutations within the vanishing twin in a few instances stop it from properly developing. The genetic abnormalities have occurred at the time of conception and cannot be prevented or regulated. The other twin absorbs the tissue of the deceased twin, and the operation is usually non-harmful to the in-utero embryo.
Why Do Identical Twins Form in the First Place?
While it is known that a fertilized egg sometimes splits to create identical twins, the underlying reasons remain a mystery. Unlike fraternal twins, whose likelihood is influenced by genetics, identical twins appear to occur randomly. Identical twinning happens at a consistent rate worldwide, approximately three to four times per 1,000 births, suggesting that factors other than genetics may play a role.
Researchers believe that epigenetic changes may be at play. Because DNA methylation is important in early embryonic development, some epigenetic alterations may determine whether an embryo divides to create identical twins. But more research is required to establish whether these epigenetic signatures are a cause, consequence, or side effect of twinning.
In order to gain more insight into identical twinning and vanishing twin syndrome, researchers intend to perform functional studies in human cells and animal models. By studying the role of epigenetic changes in embryonic development, scientists hope to determine the exact mechanisms that result in the creation of identical twins.
Moreover, scientists can broaden their research to investigate a wider variety of epigenetic changes beyond the 834 genes that have been discovered to date. As DNA methylation is only one component of epigenetic control, studying other chemical alterations may yield more insights into early embryonic development.
Emotional and Clinical Impact of Vanishing Twin Syndrome
In parents with vanishing twin syndrome, the emotional implications may be strong. While VTS cannot be prevented or treated, clinical and emotional help is important in coping with grief and enduring pregnancy.
As defined by the Cleveland Clinic, VTS is typically diagnosed by ultrasound, when an earlier visible embryo cannot be seen. Parents tend to experience a blend of emotions, weighing the excitement of a progressing pregnancy against the loss of the missing twin. Knowledge of the biological reasons behind VTS can assist in giving closure and assistance to families plagued by this condition.
Maternal Vaccination During Pregnancy Can Prevent COVID-related Hospitalization In Babies: Study

Credit: iStock/Canva
Maternal vaccination with the COVID-19 vaccine during pregnancy can be effective against severe disease and hospitalization from the SARS-CoV-2 virus in babies, according to a large study.
The study, published in the journal Pediatrics, revealed that COVID vaccination during pregnancy can protect the children against hospitalization for COVID during the first six months of life.
Also Read: COVID-19 Cicada Variant: Will It Become The Dominant Strain In The US? Know All About The Virus
Amid continuing COVID cases, babies under six months old continue to have one of the highest rates of hospitalization — one in five — due to the COVID virus in the US, as per a 2024 study.
As currently no vaccines against COVID are available for neonates and babies, the American College of Obstetricians and Gynecologists (ACOG) recommends maternal vaccination during pregnancy.
Maternal COVID Vaccination Prevented Other Infections
The retrospective study included 146,031 infants born in Norway between March 2021 and December 2023. Of these, 37, 013 (25 percent) were exposed to COVID-19 vaccination in utero.
The findings showed that babies exposed to the vaccine before birth were no more likely to visit the hospital for overall infections (of any kind) than those whose mothers did not get vaccinated in pregnancy.
However, infants whose mothers were vaccinated were about half as likely to visit the hospital specifically for COVID in their first two months of life compared to babies not exposed to the vaccine in utero.
Also Read: Olivia Munn Opens Up About Detecting No-Symptom Breast Cancer With Lifetime Risk Assessment Test
Among 3 to 5-month-old babies, the risk of a hospital visit for COVID was 24 percent lower in those exposed to the vaccine, but the vaccine's protection against COVID wore off by the time infants were older than 6 months.
Importantly, the mothers' vaccine also prevented the risk of other infections in children.
"There is often an increased risk for a subsequent infection after a viral infection, such as an increased risk of pneumonia after influenza infection, so we wanted to study whether protection against COVID-19 could influence the risk of other infections as well," said lead author Dr. Helena Niemi Eide, from the University of Oslo in Norway, the NPR reported.
"But we found that COVID vaccination in pregnancy protected the infant against COVID and had no apparent effect on other infections," Eide added.
Maternal Vaccine Recommendation in the US
Last week, the American College of Obstetricians and Gynecologists reiterated its recommendation for COVID vaccination during pregnancy.
Despite changes in federal vaccine recommendations due to the US Health Secretary Robert F. Kennedy Jr.’s anti-vaccine stance, the ACOG urged COVID vaccination for
- people who are pregnant,
- recently pregnant,
- considering pregnancy,
- lactating.
Also read: Bipolar Disorder: How Early Detection Can Help Prevent Serious Complications
"Accumulated safety data from millions of administered doses show no increased risk of adverse maternal, fetal, or neonatal outcomes associated with COVID-19 vaccination in pregnancy,” the ACOG said.
'Husband Stitch': A Medical Necessity Or Just A Tool To Objectify Women's Bodies?

Credits: AI-generated and iStock
When 36-year-old mom Angela Sanford, from Fort Mill, SC, went for an appointment for a Pap smear five years after she had her first child in 2008, her nurse midwife, who she has never seen before asked her a question she did not expect. "Who stitched you up after your first birth?"
Speaking to Healthline, Sanford shared that she just started crying when the nurse said, "This is not right." Sanford said that this was the first time she ever heard the term 'husband stitch'. Sanford was told that her stich was "too tight" by the hospitalist who managed her after her first delivery.
Also Read: US CDC Warns Of New Immune-Evasive COVID Variant In 23 Countries
“He gave you what some people call a husband stitch,” Sanford recalled the midwife telling her.
“I couldn’t connect in my mind why it would be called that. My midwife said, ‘They think that some men find it more pleasurable,’” she recalled. “My husband has been worried about me and fearful of hurting me. He would never have asked for this.”
A 'Husband Stich' - What Is It?
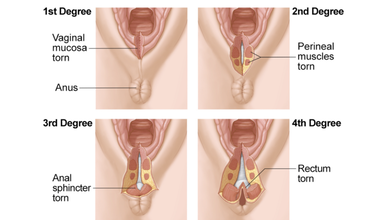
During vaginal delivery, a woman undergoes perineal tears or vaginal lacerations which means tears between the vaginal opening and anus. This causes pain, and requires stitches for grades two and higher. It also takes 4 to 6 weeks to heal. Women can experience from first to fourth degree tears.
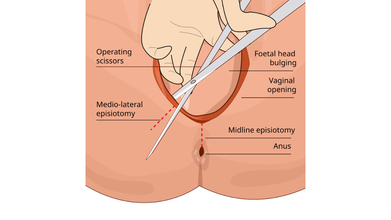
Sometimes, a surgical incision is made in the perineum during childbirth to enlarge the vaginal opening, this is called an episiotomy. However, it is not medically necessary or a routine procedure, unless it is a case of emergency.
Stiches are required in such cases that dissolves on its own. However, a 'husband stitch', also known as "daddy stitch" is an unethical practice where an extra stitch is given during the repair process that 'tightens the vagina' to increase sexual pleasure for a male partner. While it is considered a medical malpractice, it is still done to women after vaginal delivery.
Many women face difficulty after the extra stich is given to them. In Sanford's case, she felt "excruciating" pain during sex afterwards.
Read: Romanticization And The Silent Dismissal Of Women’s Pain
When Objectifying Women's Bodies Is Made A Medical Practice
Stephanie Tillman, CNM, a certified nurse midwife at the University of Illinois at Chicago and blogger at The Feminist Midwife told Healthline: “The fact that there is even a practice called the husband stitch is a perfect example of the intersection of the objectification of women’s bodies and healthcare. As much as we try to remove the sexualization of women from appropriate obstetric care, of course the patriarchy is going to find its way in there."
Harkins, 37, said that she "kind of" laughed it off when an "old, crusty Army doctor" overstitched her so she could give her husband more pleasure. In many cases, doctors do it as a routine practice without even being told by anyone. “I couldn’t even process [it], but I kind of laughed, like what else do you do when someone says that? I had just had a baby. I didn’t think much about it because the whole birth experience was so traumatizing, but now that I think about it differently, the implications of that are just crazy.”
Episiotomy Is An Excuse For 'Husband Stitch'
Dr Robert Barbieri, chair of obstetrics and gynecology and reproductive biology at Brigham and Women’s Hospital in Boston, told the Huffington Post that doctors were taught in the 50s and 60s that "routine episiotomy was good for women".
“What they thought is that if they did a routine episiotomy, they’d have a chance to repair it and that during the repair, they could actually create a better perineum than if they hadn’t done it. The idea [was] that we could ‘tighten things up,’” explains doctor.
However, a 2005 systematic review in the Journal of the American Medical Association found no benefit to routine episiotomy use. A 2017 Cochrane review “could not identify any benefits of routine episiotomy for the baby or the mother.” In 2016, the American College of Obstetricians and Gynecologists (ACOG) recommended that clinicians “prevent and manage” delivery lacerations through strategies like massage and warm compresses rather than making cuts on the perineum. Yet, this practice still continues inside the labor rooms.
Your Kids’ Fast-fashion Clothing May Be Laced With High Levels of Toxic Lead

Credit: iStock
While you may be buying fast-fashion clothes that are easy on your pocket and also give your children trendy looks, a new study highlights the risk of being laced with a highly toxic ingredient: lead.
The preliminary research, based on lab tests of several shirts from different retailers in the US, found that all the samples exceeded the country’s federal regulatory lead limits.
The US Consumer Product Safety Commission currently has a 100 parts per million (ppm) lead limit for children's products like toys and clothing.
"I started to see many articles about lead in clothing from fast fashion, and I realized not too many parents knew about the issue," said Kamila Deavers, principal investigator of the study, at Marian University in the US.
Deavers began the study after her young daughter’s lab reports showed elevated levels of lead in her blood from toy coatings.
How was study conducted?
The team tested 11 shirts that spanned the rainbow—red, pink, orange, yellow, gray, and blue. All brightly colored fabrics, particularly reds and yellows, showed higher levels of lead compared to more muted tones.
"We saw that the shirts we tested were all over the allowed limit for lead of 100 ppm," said Priscila Espinoza, from Marina.
The researchers explained that some manufacturers use lead (II) acetate as an inexpensive way to help dyes stick to the materials and produce bright, long-lasting color.
Children At Greater Risk
The researchers found the risk is particularly higher among younger kids as they tend to playfully suck or chew their clothes during play.
"Even briefly chewing these fabrics could expose children to dangerous lead levels,” they found in the study, to be presented at the forthcoming meeting of the American Chemical Society.
According to the US Environmental Protection Agency (EPA), lead exposure can lead to behavior problems, brain and central nervous system damage, as well as other negative health effects in children.
The agency considers children under six years old to be most at risk from exposure. Even low levels of lead in the blood of children can result in:
- Behavior and learning problems
- Lower IQ and Hyperactivity
- Slowed growth
- Hearing Problems
- Anemia
The researchers also pointed out safer alternatives to lead-based dyeing agents that already exist. These include natural and less harmful substances such as:
- Plant-based tannins (e.g., oak bark, pomegranate peel)
- Rosemary
- Alum.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited