- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
- Web Stories
The ‘Make America Healthy Again’ Report Is Releasing Soon: 5 Big Things It Might Reveal

Credits: Health and me
Washington is gearing up to drop part two of its “Make America Healthy Again” agenda, and expectations are high. The first MAHA assessment, delivered to the White House this spring, framed a blunt thesis — American children are getting sicker, faster, and the drivers are mostly man-made. The follow-up “Strategy” report, due to be unveiled after it’s transmitted to the White House, is supposed to move from diagnosis to action. If you care about what kids eat, breathe, watch, and are prescribed, this matters.
Below is what the first report already established, what the new one is likely to do with it, and why the battles ahead won’t be tidy.
The White House’s MAHA Assessment was explicit: the United States faces a childhood chronic disease crisis and four forces are doing the heavy lifting — ultra-processed foods, cumulative chemical exposures, inactivity and chronic stress in a digital era, and over-medicalization of kids. It also laid out the machinery: an executive order created a Commission chaired by the Health and Human Services Secretary, tasked to deliver an assessment within 100 days and a strategy within 180 days, with the President’s senior health, science, and budget leaders named as members.
A few data points stood out. The Assessment claims more than 40 percent of U.S. children have at least one chronic condition; it attributes nearly 70 percent of kids’ calories to ultra-processed foods; and it argues that regulatory gaps allow cumulative chemical exposures to stack up in ways our policies haven’t kept pace with. It also points to soaring screen time, sleep loss, and stress, and warns that a culture of “treat first, ask later” has normalized aggressive medication in pediatrics.
The White House
That framing signals where the Strategy is headed. Let’s break it down into five likely reveals.
1) A push to de-normalize ultra-processed foods in federal programs
Expect the Strategy to take aim at ultra-processed foods (UPFs) across the programs Washington controls or influences — school meals, WIC, SNAP, and federal procurement. The Assessment spends an entire section on UPFs, arguing they displace nutrient-dense foods and expose kids to additives and sweeteners that track with obesity and metabolic disease. It cites the “nearly 70 percent” figure for children’s calories from UPFs and positions whole foods as the default standard. That sets up obvious levers: revising food specifications in school nutrition, tightening allowable additives in federally funded meals, and incentivizing regional supply chains for minimally processed foods.
Here’s what that could look like in practice: higher reimbursement tiers for scratch-cooked menus; procurement standards that limit defined UPF categories; clearer front-of-package transparency tied to federal vending or contracting; and pilot funds for districts to install basic cooking capacity. Because the Assessment explicitly links diet quality with chronic disease trajectories, the Strategy will likely argue these are health spend-avoidance, not just nutrition line items.
2) Chemicals: from single-substance safety to cumulative risk
Another likely pillar is an attempt to modernize how agencies evaluate environmental exposures. The Assessment flags that children are uniquely vulnerable to a growing “aggregation” of synthetic chemicals, and suggests current frameworks don’t adequately capture cumulative or mixture effects. Translation: don’t be surprised if the Strategy proposes a cross-agency effort to incorporate cumulative risk methodology, faster review cycles for chemicals common in food contact materials or school environments, and a more aggressive stance on data transparency around exposure sources.
Politically, this is the hottest burner. Farm groups already bristled at the Assessment’s references to studies linking common pesticides with cancer and liver problems. Expect the Strategy to thread the needle: phase-ins, exemptions for certain crops, and “safer substitution” funds for growers, while still signaling a turn away from chemicals with weak pediatric safety margins. The Assessment’s section on “corporate capture” and regulatory conflicts of interest previews tougher conflict-of-interest guardrails, which could extend to advisory panels and grantmaking.
3) Digital-age health: screen time, sleep, and movement standards with teeth
The Assessment ties a “decline of physical activity,” chronic stress, rising screen use, and sleep deprivation to worsening pediatric health. If the Strategy builds on that, look for concrete targets: daily movement minutes in schools, device-free windows for homework platforms, and funding for safe routes and after-school sport access in low-income districts. It may also propose standardizing sleep education and mental health screening in pediatric primary care tied to reimbursement, treating movement and sleep as vital signs rather than nice-to-haves.
To avoid culture-war potholes, the Strategy will likely focus on harms that enjoy broad consensus — sleep debt, musculoskeletal issues, sedentary behavior — rather than content moderation. Still, you can expect language urging “age-appropriate design” and data-minimizing defaults for platforms used in schools.
4) Reining in over-medicalization: audit the incentives, elevate prevention
One of the Assessment’s most provocative claims is that American children are “on too much medicine,” driven in part by research, regulatory, and clinical incentives that reward treatment over prevention. That sets the stage for a Strategy that asks payers to reimburse prevention like care: nutrition counseling, family-based lifestyle interventions, metabolic screening for high-risk kids, and deprescribing reviews. Expect pilots that tie Medicaid and CHIP dollars to prevention outcomes, encourage collaborative care models, and require pediatric-specific evidence for high-volume prescribing categories.
Don’t be surprised if the Strategy also calls for stronger disclosure and firewall rules around financial conflicts in guideline writing and clinical education, consistent with the Assessment’s “revolving door” critique. The goal is not to stigmatize necessary medicine, but to flip default settings so the first move is to address root causes when appropriate.
5) A whole-of-government playbook — with deadlines and dashboards
The Assessment is clear about timelines: the Commission delivers an Assessment, then a Strategy. The Strategy’s credibility hinges on measurable targets, agency owners, and public reporting. Expect a “whole-of-government” matrix that assigns tasks to HHS, USDA, EPA, Education, VA, OMB, OSTP, and FDA leadership — the very roles listed in the Assessment — with 6-, 12-, and 24-month deliverables. Think: a public dashboard tracking UPF prevalence in school meals, children’s exposure biomarkers in national surveys, physical activity minutes, and antibiotic or stimulant prescribing trends in pediatrics.
Given the White House’s emphasis on “radical transparency” in the Assessment — and its explicit statement that the Strategy must be “grounded in a common scientific basis” — the rollout may include commitment to open datasets, independent replication grants, and rapid-cycle pilots with third-party evaluation. That’s how you translate rhetoric into durable policy.
The White House
What Could Spark The Biggest Debates And Controversies?
Two flashpoints are already visible. First, agriculture and chemical policy: any move perceived as undermining pesticide tools or vilifying mainstream farming will face hard pushback. Second, the food industry: voluntary pledges to tweak recipes won’t cut it for nutrition advocates, but mandatory standards risk court challenges and supply-chain friction. The Strategy’s reception will hinge on whether it pairs higher standards with real transition help — procurement guarantees for farmers, grants for school kitchens, and a phase-in timeline that’s realistic.
On screens and stress, expect fewer fireworks — parents, clinicians, and schools largely agree kids need more sleep and movement — but the implementation details matter. Unfunded mandates will stall; funded pilots with clear metrics can move.
How To Read The Report When It Releases?
When the Strategy drops, skip the slogans and scan for five things: specific agency actions, measurable targets, funding sources, timelines, and independent evaluation. If those are present — and aligned with the Assessment’s four drivers — you’re looking at more than a press conference.
If they’re vague, the headline risk is that the Strategy becomes another well-intended framework that fades by the next budget cycle.
The MAHA Assessment argued that kids’ health is failing not because we lack medical breakthroughs, but because daily exposures — to engineered foods, chemicals, screens, stress, and quick-fix prescribing — have outpaced our policies. The Strategy’s job is to reverse that equation with rules, incentives, and transparency that make the healthy choice the default in schools, clinics, and communities. If it delivers clear standards for food, modernized chemical risk policies, funded movement and sleep initiatives, and a rebalanced payment system that rewards prevention, it could mark a real turn.
XFG ‘Stratus’ COVID Now Dominant in US: States With Highest Cases and How to Spot Unique Symptoms

Credits: Canva
The XFG “Stratus” COVID-19 variant is officially strutting into the pandemic spotlight. It is new, it is bold, and according to the latest data from the Centres for Disease Control and Prevention (CDC), it is now the third most common variant in the US. But it is popping up in certain states more than others, and the way it announces its arrival could be by making your throat feel like you have swallowed a box of sandpaper.
While the national Covid-19 test positivity rate sits in the 5–9.9 per cent range, a dozen states are seeing significantly higher numbers.
According to CDC data, the states with the highest positivity rates are:
- New Mexico (12%)
- Texas (12%)
- Oklahoma (12%)
- Arkansas (12%)
- Louisiana (12%)
- Nevada (11.3%)
- Arizona (11.3%)
- California (11.3%)
- Alaska (11.1%)
- Washington (11.1%)
- Oregon (11.1%)
- Idaho (11.1%)
These states are not just reporting higher numbers but are also providing ideal conditions for Stratus to spread. With case trends officially “growing” according to the CDC, it is a situation that demands close attention.
Stratus is a variant under monitoring by the World Health Organisation (WHO). First detected in January, XFG Stratus now accounts for about 14 per cent of Covid cases in the US.
While theW says the health risk from Stratus remains low at a global level, this variant is still on a growth spurt, outpacing other circulating forms of the virus, including its sibling, the “Nimbus” NB.1.8.1 variant. The concerning bit is that the WHO says Stratus could be more adept at sidestepping immune defences. The reassuring bit is that the current vaccines are expected to continue protecting against symptomatic and severe disease caused by Stratus.
Spotting Unique Stratus Symptoms
The tricky thing about Stratus is that it is not trying to reinvent the Covid symptom wheel. According to experts, its symptoms look suspiciously similar to other recent Omicron descendants. But there is one possible stand-out, a sensation some patients are calling “razor blade throat”.
Here’s the full checklist:
- Sore throat (sometimes severe)
- Cough
- Congestion or runny nose
- Fever or chills
- Shortness of breath
- Loss of taste or smell
- Fatigue
- Headache
- Muscle aches
- Nausea, vomiting or diarrhoea
The “razor blade throat” description might sound too much, but anyone who has had that burning, scratchy pain knows it is no joke. Hoarseness has also been reported more often lately. Still, a sore throat has been a hallmark Covid symptom since the early days of the pandemic; Stratus just seems to be leaning into it.
Why the Positivity Spike Matters
Higher positivity rates do not just mean more people are testing positive; they can also signal under-testing. If more than 10 per cent of people tested are infected, it suggests many cases are flying under the radar, which means more opportunities for the virus to spread unchecked. That is especially risky when you have a variant with a knack for growing its share of cases quickly, like Stratus.
The fact that 12 states are sitting above the 11 per cent mark means public health teams will be watching these regions closely in the coming weeks. In the meantime, everyday precautions like masking in crowded places, testing if symptomatic, and staying up to date with vaccines remain the best tools in the toolbox.
Stratus vs. Nimbus
While Stratus is currently the one hogging headlines, it is not alone. The “Nimbus” NB.1.8.1 variant is still in the mix, though it is being outpaced by Stratus globally.
For now, Stratus is the one to watch and not because it is the most dangerous, but because it is the fastest climber.
Final Forecast
The XFG Stratus variant is not changing anything, but it is a reminder that the virus is still evolving and still finding ways to make itself known. Got a sudden sore throat that feels like sandpaper? Do not brush it off. Stratus may not be a storm you can see on a weather map, but it is definitely in the air.
UK Health Chiefs Warn of Rising Cases of Deadly Chikungunya Virus That Can Cause Body to ‘Fold In on Itself’

Credits: Canva
Health authorities in the UK have reported a significant rise in chikungunya cases, a mosquito-borne disease known for causing severe joint pain that can leave sufferers hunched over. Between January and June 2025, there were 73 confirmed cases in England, Wales, and Northern Ireland, more than double the 27 recorded during the same period in 2024. The UK Health Security Agency (UKHSA) says this is the highest number ever recorded, with nearly all linked to overseas travel.
What is Chikungunya?
Spread by the bite of infected Aedes mosquitoes, particularly the Aedes aegypti and Aedes albopictus species, chikungunya is not usually deadly but can be devastating for the very young, the elderly, or those with underlying health conditions.
Typical symptoms include:
- Excruciating joint pain that can leave sufferers bent over in agony
- High fever and headaches
- Muscle aches and swelling in the joints (especially hands and feet)
- Nausea, fatigue, and a rash that’s red, bumpy, and decidedly not Instagrammable
In severe cases, the arthritis-like pain can linger for months or even years, turning every movement into a reminder that mosquitoes are not just a mild holiday nuisance.
The majority of UK cases this year were linked to travel to Sri Lanka, India, and Mauritius. All were reported in England, with London taking the dubious honour of having the most cases. However, the two mosquito species that spread the virus are not established in the UK, so there is no risk of it transmitting locally.
UK logs first cases of oropouche virus
As if one virus was not enough, the UK has also logged its first cases of the oropouche virus, also dubbed ‘sloth fever’. This one circulates in the wild between primates, sloths, and birds before occasionally hopping over to humans via midges or mosquitoes.
Found primarily in the Amazon basin, oropouche has recently started wandering further across the Americas. All the UK cases were linked to travel from Brazil, so unless your staycation involves tree-dwelling mammals and tropical insects, you are safe for now.
The Global Bug Crawl
Chikungunya is typically found in Africa and southern Asia, but 2025 has seen it pop up in unexpected places. Outbreaks have been reported in China, the Indian Ocean islands of Reunion, Mayotte and Mauritius, and across the Americas. In southern China, more than 7,000 people have been infected since June, prompting COVID-style lockdowns in Foshan and at least a dozen other cities in Guangdong province. Hong Kong and Taiwan have also reported cases.
Health officials are urging travellers to take bite prevention seriously.
How to safeguard against mosquito bites
According to the US Centres for Disease Control and Prevention (CDC), your best defence is to stop mosquitoes from making contact in the first place.
Top tips include:
- Use Environmental Protection Agency (EPA)-registered insect repellent
- Wear long-sleeved shirts and trousers (mosquitoes can’t bite what they can’t reach)
- Treat clothing and gear with 0.5% permethrin for extra armour
- Choose accommodation with air conditioning or window screens
- If sleeping outdoors, use a mosquito net unless you enjoy sharing your bed with the local insect population
Vaccination
In addition to covering up and dousing yourself in repellent, some travellers may be advised to get the chikungunya vaccine before heading to certain destinations. Your healthcare provider can help you decide if this applies to your travel plans.
Why the Surge Now?
Several factors could be behind the sharp rise in cases. Increased international travel post-pandemic, changing weather patterns favouring mosquito breeding, and outbreaks in popular holiday destinations have created a perfect storm. Mosquitoes thrive in warm, wet conditions, and with climate change extending those conditions into more regions, these viruses are no longer staying politely within their old borders.
Chikungunya virus can turn a dream getaway into a painful endurance test, and once contracted, it is all about managing symptoms; there is no cure. The same goes for oropouche: prevention is your best friend. In the world of tropical diseases, an ounce of repellent really is worth a pound of cure.
Scott Swift, Taylor Swift's Dad Underwent A Quintuple Bypass Heart Surgery, Here's What We Know About It So Far
Credits: Treemily
Scott Swift, 73, pop singer Taylor Swift's dad just underwent a quintuple bypass surgery, revealed Taylor during one of the episodes of Travis Kelce and Jason Kelce's New Heights podcast.
She also shared that she had moved in with her dad earlier this year to take care of him for a speedy recovery. She noted that her father has been full of gratitude after the surgery. "He was the loveliest patient ever. He just kept saying thank you over and over again."
Why Did Scott Swift Need A Surgery?
Taylor called the surgery "really intense" and said that her dad's heart always had a healthy ECG or electrocardiogram. He also ensures to get it every year to remain a step ahead of any physical ailments. However, five hard blockages were found in his heart during a resting stress test.
"He's been telling all his friends, 'You need to get the stress test,' because that's what's actually preventative. If you can find that earlier, you don't have to have a bypass surgery," she said.
Taylor confirmed that her father is doing "incredibly well" and that his humor has helped him go through during the hard times. It still is very much intact in him.
She shares that he did not know how many blockages he's had, on being told that he underwent a quintuple bypass, which means five blockages, he also joked about it. "Well, you see, I come from a very competitive family," he told Taylor.
What Is A Stress Test?
As per the National Institute of Health (NIH), US, it is a form of physical test that typically utilizes electrocardiography along with blood pressure monitoring and exercise, which involves a treadmill or bicycle.
However, in a resting stress test, the assessment happens when the heart muscle is at rest after stress. This stress helps in identifying areas of reduced blood flow like ischemia or damage to the heart muscle, which can indicate conditions like coronary artery disease.
The test involves injecting a radioactive tracer into the bloodstream, then using a special camera to take images of the heart at rest and after stress.
What Is A Bypass Surgery?
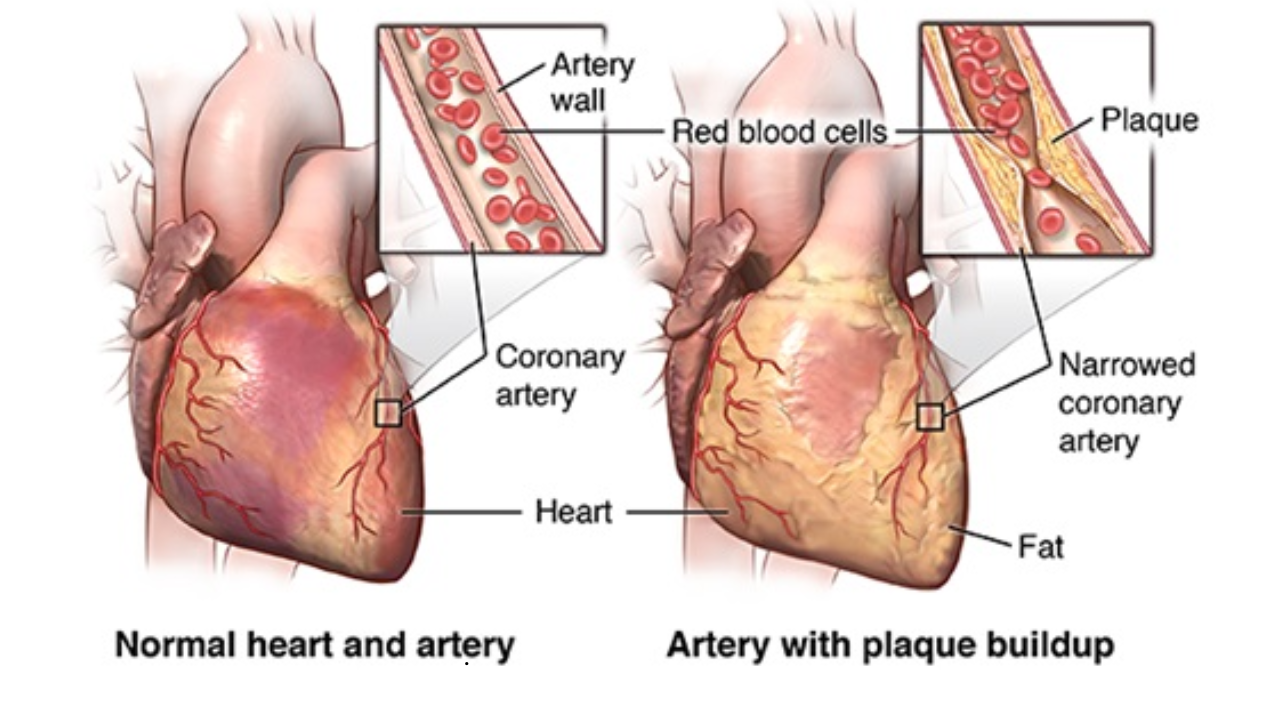
As per Johns Hopkins Medicine, bypass surgery or coronary artery bypass graft surgery (CABG) is a procedure used to treat coronary artery disease. Coronary artery disease (CAD) is the narrowing of the coronary arteries. These are the blood vessels that supply oxygen and nutrients to the heart muscle. CAD is caused by a build-up of fatty material within the walls of the arteries. This buildup narrows the inside of the arteries, limiting the supply of oxygen-rich blood to the heart muscle.
How Does It Work?
One way to treat the blocked or narrowed arteries is to bypass the blocked portion of the coronary artery with a piece of a healthy blood vessel from elsewhere in your body. Blood vessels, or grafts, used for the bypass procedure may be pieces of a vein from your leg or an artery in your chest. An artery from your wrist may also be used.
ALSO READ: 4 Rare Heart Diseases That Are Becoming Common By Each Passing Day
This surgery is done to treat a blockage or narrowing of one or more of the coronary arteries. It can restore the blood supply to your heart muscle when nonsurgical procedures are not a choice.
More Updates From The Swift Family
In addition to Scott, Taylor shared that her mom Andrea Swift, too, under a procedure. “My mom just got a new knee,” Taylor shared. “She’s doing great. She’s scampering around. We’re not quite at scampering yet, but she’s doing great.”
She noted that her parents are her best friends.
"It was actually one of the most special things that's ever happened to me, spending all that time with them this summer. You have those long talks that you don't have when it's a small, concentrated period of time.”
- Follow Us :



© 2024 Bennett, Coleman & Company Limited