- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
This Simple Eye Test Could Save You From Stroke, New Study Suggests

Image Credit: Canva
The human eye has long been considered a window to the soul, but modern science reveals its potential for being a diagnostic window toward our health. Researchers have already discovered that in the retina – the light-sensitive layer at the back of the human eye – resides an intricate network of blood vessels that can foretell crucial elements about a person's risk to stroke. This finding is a non-invasive and accessible approach to predicting stroke, hence challenging the dependency on the classic risk factors alone, such as high cholesterol or blood pressure. Recent research published in the journal Heart identified a "vascular fingerprint" in the retina, comprising 29 indicators of blood vessel health.
This fingerprint can predict the likelihood of a stroke with accuracy comparable to conventional methods. These indicators include characteristics like the density, twistedness, and complexity of retinal veins and arteries, which mirror the vascular architecture of the brain.
This innovative approach is particularly promising for primary healthcare settings and resource-constrained environments, where invasive lab tests may not be feasible. The potential to assess stroke risk through a simple retinal scan marks a significant leap in preventive medicine.
The researchers, who include those from The Royal Victorian Eye and Ear Hospital in Australia, analyzed fundus images, which are specialized photographs of the retina from more than 68,000 participants in the UK Biobank dataset. Over an average follow-up period of 12.5 years, 749 of those participants had a stroke.
The researchers used advanced machine learning models, such as the Retina-based Microvascular Health Assessment System (RMHAS), to study 30 indicators in five key categories of retinal vascular architecture.
These categories included calibre, which measured the length, diameter, and ratio of veins and arteries; density, which focused on the distribution of blood vessels in the retina; twistedness, analyzing the curvature and patterns of the vascular network; branching angle, which examined how veins and arteries split into smaller branches; and complexity, which evaluated the overall intricacy of the vascular network. In the study, age, sex, socioeconomic status, lifestyle habits, and health parameters, including blood pressure and cholesterol levels, were taken into account to ensure that the findings were robust. The analysis showed that 29 out of 118 retinal vascular indicators are significantly associated with first-time stroke risk.
Changes in density indicators corresponded to 10-19% increased risks of stroke; alterations in calibre indicators were accompanied by a 10-14% increase. Other studies have suggested that decreases in complexity and twistedness indicators corresponded to a 10.5-19.5% higher risk of stroke. These data support the retinal imaging non-invasive diagnostic tool for prediction of early stroke.
Amazingly, the retinal vascular fingerprint alone, in combination with only age and sex, was as good at predicting stroke risk as traditional methods that rely on invasive tests.
How the Retina is Connected to your Brain
Retinal blood vessels bear anatomical and physiological resemblance to those in the brain. Given this, it is an attractive organ for understanding the systemic health of the vasculature. Many diseases, for example, which damage blood vessels throughout the body, leave evidence in the retinal microvascular network. Diabetic retinopathy and hypertensive retinopathy are examples.
The study does have several limitations with this being an observational research, and so it cannot claim to establish any cause-and-effect relationships. The research was also primarily conducted on whites, which makes the findings a little less generalizable to a diverse population. Future studies would be better in including a range of ethnicities and exploring the risk of stroke associated with the type of stroke.
Simple Method To Detect Stroke Risk
Traditional stroke risk assessment is often confined to blood studies and imaging studies; however, these tools are not freely available in some low-resource settings. Retinal photography provides a completely non-invasive imaging modality. All that will be needed will be a basic photograph of an eye.
It is, therefore, through the introduction of artificial intelligence that has been a game-changer in retinal imaging. Systems like RMHAS rely on machine learning to pick out patterns and biomarkers that the human eye might not identify. Such improvements not only enhance predictive accuracy but also speed up the process while making it more cost-effective.
Also Read: 3 Shocking Stroke Risk Factors You Need To Control NOW
Prevention of Stroke through Early Detection
Stroke is one of the leading global health concerns, causing nearly 100 million cases a year and killing 6.7 million people. The majority of the cases are due to modifiable risk factors, including high blood pressure, poor diet, and smoking. The early warning system could help individuals and healthcare providers act proactively on these risks by providing an early warning system.
The discovery of the vascular fingerprint of the retina as a predictor of stroke risk is a testament to the power of innovative diagnostics. This non-invasive, accessible method may revolutionize stroke prevention, especially in underserved communities. As research continues to refine this approach and broaden its applicability, the eye may soon become an essential tool in safeguarding our brain health.
Every Day Tips to Prevent Stroke and Detect Risks Early
The good news is that strokes can be prevented in most cases by living a healthy lifestyle, coupled with knowing the early warning indicators. Implement these tips daily and prevent your risk for stroke before it gets too late.
- High blood pressure is one of the leading risk factors for stroke. Uncontrolled hypertension can weaken blood vessels, making them more prone to rupture or blockage. Invest in a home blood pressure monitor to check your readings regularly. Maintain a target of 120/80 mmHg by reducing salt intake, staying physically active, and adhering to prescribed medications.
- Unhealthy eating habits, such as diets with high levels of processed foods, saturated fats, and cholesterol, can lead to obesity and blocked arteries. A diet rich in fruits, vegetables, whole grains, lean protein, and healthy fats is key. Include leafy greens, berries, nuts, and fish high in omega-3s, which help maintain cardiovascular health.
- Regular physical activity lowers the risk of high blood pressure, obesity, and diabetes, three leading causes of stroke. Try to engage in at least 150 minutes of moderate-intensity aerobic activity a week. Examples include brisk walking, cycling, or swimming. Also incorporate strength training to help strengthen your blood vessels.
- Smoking harms your blood vessels, promotes blood clots, and reduces the oxygen in your blood. Overconsumption of alcohol can raise your blood pressure and lead to weight gain. Quit smoking with support groups, counseling, or nicotine replacement therapy. Limit your intake of alcohol to moderate levels; that is, one drink a day for women and two for men.
- Unmanaged conditions, such as diabetes, high cholesterol, and atrial fibrillation, significantly increase stroke risk. Work with your healthcare provider to monitor and manage these conditions. For example, maintain blood sugar levels within target ranges for diabetes and take anticoagulants if diagnosed with atrial fibrillation.
- Obesity strains the cardiovascular system and increases the risk for stroke. Have a healthy diet along with regular exercise to have a sustainable weight loss. Small, consistent changes in, say, portion control or simply not having too many sugary drinks may make a big difference.
- As a result of this, dehydration could thicken blood, then clots might form. Drink at least 8-10 glasses of water per day. Include hydrating foods like cucumbers and watermelon in your diet, especially during hot weather or exercise.
- Poor sleep quality increases blood pressure, triggers inflammation, and raises stroke risk. Ensure 7-8 hours of sleep at night. Develop a bedtime routine: reduce screen time, have a regular schedule, and avoid caffeine close to bedtime.
- Acting fast during a stroke can prevent long-term damage and save lives. Learn the FAST acronym:
F: Face drooping
A: Arm weakness
S: Difficulty speaking T: Time to call 911
- Regular medical check-ups can identify and manage stroke risk factors before they lead to a stroke. Make an annual physical to track cholesterol, blood pressure, and other essential health markers. If you have a family history of stroke, discuss retinal imaging or carotid artery screening with your physician.
Retinal vascular fingerprints predict incident stroke: findings from the UK Biobank cohort study. Heart. 2025
Amanda Peet Opens Up About Breast Cancer Battle, Shares Toughest Moment

Credit: Instagram
Amanda Peet, the Hollywood actress known for roles in Something’s Gotta Give, The Whole Nine Yards, and Jack & Jill, recently opened up about her breast cancer diagnosis and how informing her kids about her health became the toughest part for her.
In a New Yorker essay published March 21, the 54-year-old actress announced how a routine scan in August 2025 showed an unusual ultrasound result. Later, a biopsy detected a tumor that “appeared” small.
The Dirty John star found to be in stage 1 of lobular cancer that is “hormone-receptor-positive” and “HER2-negative,” making her “happier than the pre-diagnosis” stage.
It is because Hormone-receptor-positive and HER2-negative cancer is less aggressive and often easier to treat than more aggressive forms of breast cancer.
However, informing her children, Frances, 19, Molly, 15, and Henry, 11, about the cancer was the toughest part for her, and she had to be in the right mindset before sharing the news with them.
“They've been great,” Peet told E! News.
“I definitely had to get myself together before including them. The hard part was realizing that nothing is certain and there was going to be no perfect time to tell them,” she added.
Peet stated that between her diagnosis, she had also been navigating a series of family health crises — with both of her parents' final months in hospice care.
The Your Friends & Neighbors actress, in her essay, also noted that she would “only need a lumpectomy and radiation,” not a double mastectomy.
What is Lobular Cancer?
Invasive Lobular Carcinoma (ILC) the second most common form of breast cancer, representing 5 to 15 percent of breast cancer cases.
Rather than a distinct lump, it can appear as a thickening or "fullness" rather than a tumor.
It is often difficult to detect on mammograms, thus MRI or ultrasound are more effective for detection
It is usually hormone receptor-positive.
What Is Hormone receptor-positive (HR+) and HER2-negative (HER2−) Breast Cancer
HR+ and HER2− breast cancer is the most common subtype and is seen among 60–75 per cent of cases.
It is not two different cancers, but rather specific, defining characteristics of the same cancer type (breast cancer). It grows:
- due to hormones estrogen/progesterone,
- lacks excess HER2 protein,
- it can occur in either or both breasts
- has a better prognosis
- slower growth rate
- often treated with hormone therapy and sometimes chemotherapy.
Why Early Diagnosis Matters for Breast Cancer
According to the Centers for Disease Control and Prevention (CDC), breast cancer screening is a proactive checkup used to find cancer before any physical signs or symptoms appear. While screening doesn’t prevent cancer, its goal is early detection, making the disease much easier to treat.
Since every person’s body and history are different, you and your doctor should engage in informed and shared decision-making. This means discussing the pros and cons to decide together if, and when, screening is right for you.
The US Preventive Services Task Force (a group of national medical experts) provides guidelines based on the latest research:
Average Risk
Women aged 40 to 74 should generally get a mammogram every two years.
High Risk
If you have a family history or other risk factors, your doctor may recommend a different schedule or additional tests.
GLP-1 Drugs: Why India Needs Stricter Rules Now

Credit: iStock
GLP-1 receptor agonists are a modern class of medicines that have changed the treatment of type 2 diabetes and obesity. In simple terms, they help the body respond to food more smartly. After eating, the intestine naturally sends signals that help regulate sugar and appetite levels.
GLP-1 RA medicines imitate this signal. As a result, blood sugar rises less after meals, appetite becomes more controlled, and many people feel full with smaller amounts of food. This is why these medicines are used not only for diabetes, but also for weight reduction in selected people.
GLP-1 Drugs: Not A Miracle Injection
These medicines are important because their benefits can go beyond sugar control alone. Studies and current diabetes guidelines show that some GLP-1 RAs can reduce body weight, improve long-term sugar levels, and lower the risk of major heart-related problems in people who have type 2 diabetes and high cardiovascular risk.
Recent guidance also supports their use in some people with chronic kidney disease when cardiovascular risk reduction is an important goal. This does not mean every drug in the group is identical, but it means the class has become medically important for more than just lowering sugar.
For the general public, one important point is that these are not “miracle injections.”
They work best when combined with better food choices, regular walking or exercise, good sleep, and medical follow-up. They are usually started slowly because the commonest side effects are stomach-related, such as nausea, vomiting, constipation, loose motions, or a feeling of fullness.
Not everyone is suitable for them, and the decision depends on a person’s diabetes status, weight, heart or kidney disease, other medicines, and cost. Used properly, GLP-1 RAs are powerful tools that can improve health, but they should always be taken under medical supervision.
GLP-1 Drugs: Urgent Need to Curb Misuse
So Indian Medical Association (IMA) is planning to seek a mandate restricting prescriptions of GLP-1 drugs to certified endocrinologists/diabetologists or MD general medicine practitioners to curb indiscriminate use and safeguard patient safety as access expands, many media report in August last year about rampant misuse of GLP1 weight loss drugs by cosmetologists, physiotherapists, dermatologists, general MBBS clinicians, and even ayurveda, and other non-modern medicine practitioners.
Many MBBS, physiotherapists, and non-modern medicine practitioners are prescribing GLP1 drugs to people who neither have diabetes nor any comorbidity or acute obesity, but purely for cosmetic reasons to lose some weight that can be otherwise easily done with some lifestyle changes like exercise and diet.
It is a duty of the government to take care of it because there is a lot of misuse and misprescription that needs to be curbed immediately, because these medicines also have side effects.
We will write to the government to take necessary action to stop the misuse of the drug. We will discuss it in our meeting in the first week of April 2026.
1 In 4 Diabetic Patients in India Suffer from Liver Fibrosis, Finds Lancet Study
Credit: iStock
One in four or 25 percent of adults with type-2 diabetes in India also suffer from liver fibrosis, according to an alarming study published in The Lancet Regional Health Southeast Asia journal today.
With data from more than 9,000 patients across the country, it is the largest ever real-world survey of liver fibrosis in type 2 diabetes from any low- or middle-income country.
While fatty liver disease has been touted as the most common liver condition among diabetes patients, the new study established liver fibrosis as the real danger among people with high blood sugar.
“Type 2 diabetes is closely linked to fatty liver disease (also known as MASLD). But how common is liver Fibrosis — the real danger — in Indian diabetics? Our answer: 1 in 4 has clinically significant liver fibrosis. One in 20 already has probable cirrhosis. Most had no symptoms. We propose liver fibrosis as the ‘4th major complication’ of diabetes,” said Ashish Kumar, from Ganga Ram Postgraduate Institute of Medical Education and Research (GRIPMER), from Sir Ganga Ram Hospital, in a post on social media platform X.
What Did The Study Find?
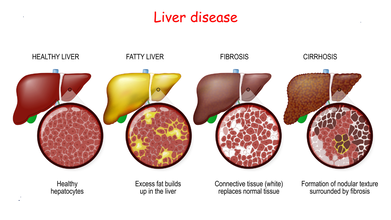
Fatty liver is typically the first and reversible stage of liver disease, where excess fat builds up in liver cells. Left untreated, it progresses to liver fibrosis, which is the excessive accumulation of scar tissue (collagen) in the liver resulting from chronic inflammation. The condition then progresses to the third and late stage, irreversible scarring (fibrosis) of the liver. The final stage is liver cancer.
The DiaFib-Liver Study included a total of 9,202 adults with type-2 diabetes patients who underwent FibroScan (VCTE) to assess liver fibrosis in routine diabetes care.
Of these:
- 26 percent had clinically significant fibrosis,
- 14 percent had advanced fibrosis,
- 5 percent had probable cirrhosis
- 65 percent had fatty liver disease.
- obesity
- dyslipidaemia
- kidney problems
- diabetes duration ≥10 years.
Fibrosis: The Screening Target
The study suggested the urgent need to integrate fibrosis screening into national diabetes programs.
“One in four adults with type 2 diabetes in India has clinically significant liver fibrosis and one in twenty already has probable cirrhosis, establishing advanced liver disease as a 'fourth major complication' of diabetes,” said the researchers.
“The DiaFibLiver Study calls for: Fibrosis — not steatosis — as the screening target. FibroScan integration into routine diabetes care. Moving beyond ultrasound-based referral,” Jha said.
“We hope this data from India adds to the global conversation on diabetes and liver disease,” he added.
Also read: The Silent Rise of Fatty Liver Disease: How India-Specific Guidelines Can Help
The findings highlight the urgent need to:
- move beyond steatosis
- systematically integrate fibrosis assessment into routine diabetes care,
- deploy non-invasive tools such as vibration-controlled transient elastography (VCTE) in community practice
- define screening strategies,
- evaluate therapeutic interventions.
Everyday Habits That Harm the Liver
Certain lifestyle choices can accelerate liver damage, such as:
Overeating processed or fried foods
High sugar intake (soft drinks, sweets, desserts)
Physical inactivity or prolonged sitting
Ignoring health issues like diabetes or hypertension
Crash dieting or taking unprescribed supplements.
How To Improve Liver Health?
Early screening and detection are key to prevent irreversible stages. Yet liver disease can be prevented with lifestyle changes such as:
- Eating a balanced diet with vegetables, fruits, whole grains, and lean protein
- Engaging in at least 30 minutes of exercise daily
- Staying hydrated to help the liver flush out toxins
- Avoiding alcohol and smoking
- Avoiding self-medication and unnecessary pills
- Getting routine health screenings.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited