- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
If You’ve Never Smoked, Why Are You At Risk For Lung Cancer?

Lung cancer is usually blamed on smoking, but a significant number of instances occur in non-smokers who have never seen the inside of a cigarette package. The American Cancer Society says that about 20% of lung cancer deaths occur in non-smokers. This leads us to ask: why are these non-smokers getting lung cancer, and why are they at risk?
Though smoking is still the primary cause of lung cancer, studies indicate that environmental, genetic, and occupational factors combined are also responsible for the development of the disease. The MD Anderson Cancer Center and other research facilities throughout the U.S. have been conducting intensive research into why lung cancer affects non-smokers and how the disease differs from smoking-induced cancer.
The majority of lung cancers that are diagnosed in never-smokers are non-small cell lung cancers (NSCLC), accounting for approximately 85% of all lung cancers. Of these, adenocarcinoma is the most frequent subtype among non-smokers. Scientists have found that close to 30% of NSCLC occurrences among non-smokers are caused by genetic mutations, which can be treated with targeted therapies.
Key Genetic Factors in Non-Smoker Lung Cancer Cases
Lung cancer in people who have never smoked is typically associated with particular genetic mutations. Two of the most important biomarkers are:
EGFR mutations: EGFR mutations account for approximately 10-15% of lung cancer in the U.S. and are more frequently found in non-smokers, especially in females and Asian patients.
ALK gene rearrangements: This mutation is found in approximately 5% of lung cancers and can be treated with certain drugs that inhibit the activity of the abnormal protein.
These genetic determinants suggest that non-smoker lung cancer patients could be more responsive to targeted therapies, bringing new hope to treatment possibilities.
Environmental and Occupational Risk Factors
Even though one does not smoke, most are exposed to substances that cause lung cancer. There are various environmental and occupational causes that have been discovered:
Radon Exposure
Radon is a naturally occurring radioactive gas that emanates from the ground and can build up in houses, particularly in basements and poorly ventilated areas. The U.S. Environmental Protection Agency (EPA) estimates that radon exposure leads to approximately 3,000 lung cancer deaths each year. Research has established a strong link between elevated radon levels and lung cancer among non-smokers.
Why is Secondhand Smoke A Significant Threat?
Even for someone who never smoked, years of exposure to secondhand smoke greatly raises lung cancer risk. According to the Centers for Disease Control and Prevention (CDC), there are an estimated 7,000 deaths from lung cancer every year due to secondhand smoke. Smokers' partners, family members, and colleagues are particularly susceptible to breathing in dangerous chemicals from cigarette smoke.
Air Pollution and Industrial Toxins
Long-term exposure to air pollution, such as vehicle exhaust and industrial emissions, has been associated with a higher risk of lung cancer. A 2013 report by the International Agency for Research on Cancer (IARC) identified outdoor air pollution as a carcinogen, highlighting the contribution of fine particulate matter (PM2.5) to lung cancer.
Exposure to these substances in the workplace, such as asbestos, arsenic, and diesel exhaust, also puts one at greater risk. People who work in construction, manufacturing, and mining are especially susceptible to inhaling these cancer-causing particles.
Family History and Genetic Susceptibility
Family history of lung cancer in non-smokers also places them at greater risk, with a possible genetic component. In case a first-degree relative (parent, sibling, or child) has developed lung cancer, especially at a younger age, the risk factor for developing the disease is elevated. This also points to inherited genetic mutations potentially making some individuals more vulnerable to lung cancer.
Identifying Symptoms
Symptoms of lung cancer are usually mild and may be confused with other illnesses, so it is frequently diagnosed late in the majority of instances. The usual symptoms are:
- Chronic cough or increasing cough over time
- Sputum containing blood
- Chest discomfort or pain
- Shortness of breath or difficulty breathing
- Wheezing
- Weight loss without an obvious cause
- Weakness
- Hoarseness or swallowing difficulty
- Recurrent infections of the lungs
Since non-smokers usually do not see themselves as being at risk for lung cancer, they might postpone medical care until the disease advances to a severe stage before being diagnosed.
Can You Lower Your Risk of Lung Cancer?
Though some risk factors, like heredity, cannot be modified, there are a number of proactive measures that you can do to reduce your risk of lung cancer. One of the most significant steps is to have your home tested for radon, as the Environmental Protection Agency (EPA) highly recommends, particularly in high-radon areas. Long-term exposure to this odorless gas can cause a high risk of lung cancer, and early detection is vital. Also, staying away from secondhand smoke is crucial. If you reside with a smoker, persuading them to quit or having proper ventilation to reduce exposure can safeguard your lungs. Lessening exposure to toxic pollutants is another crucial step—sitting indoors with air purifiers and using protective masks while working in risk-prone places can reduce the inhalation of harmful chemicals.
Lastly, a healthy way of life plays an important part in lung health. A healthy diet of fruits and vegetables, exercise regularly, and refraining from known carcinogens can make your immune system strong and help lung function in general. Using all these preventive steps can contribute significantly to lowering the risk of lung cancer and improving respiratory health. Who is Eligible for Lung Cancer Screening?
Today the U.S. Preventive Services Task Force screens for lung cancer only in individuals with a smoking history. What this implies is that non-smokers are usually not screened, except when there are symptoms or other risk indicators. There is an argument though that those who have a large family history and high exposure to radon are also worth early screening.
Lung cancer is not solely a disease of smokers. With increasing incidence in non-smokers, it's essential to know about different risk factors and take preventive action wherever feasible. If you have persistent symptoms, see your doctor to eliminate any possible serious conditions. Early detection is the strongest defense against lung cancer, irrespective of smoking status.
US Cardiologist Explains Why 2026 AHA Cholesterol Guidelines Recommend Starting Young
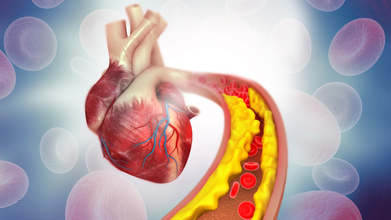
Credit: iStock
Early monitoring among younger populations has been the primary focus of the recently released American Heart Association (AHA) 2026 cholesterol guidelines.
The deliberate shift is reportedly based on new evidence about how heart disease develops over time.
Speaking exclusively to HealthandMe, Dr. Nils P Johnson, Professor of Cardiology, University of Texas, Houston, US, shared that atherosclerosis, or the buildup of plaque in arteries, doesn’t suddenly appear in middle age; it begins silently in youth.
That is why the AHA guidelines highlighted the importance of early screening.
“Cholesterol risk is really about long-term exposure. Just like years of breathing polluted air can damage your lungs, cholesterol builds up in the body over time. It’s not just about how high your levels are at one moment—it’s about how long you’ve lived with them. For example, one person might have very high cholesterol for 30–40 years, while another has moderately elevated levels for 60 years. Over time, their total exposure can be similar—and so can their risk," Dr. Johnson said.
What this means in practice is that treating cholesterol is about reducing total lifetime exposure.
The cardiologist explained that there are two ways to do that: lower cholesterol levels or start treatment earlier.
"Both approaches achieve the same goal—shrinking the overall ‘cholesterol burden’ by reducing how much cholesterol is in the body and how long a person is exposed to it,” the expert said.
The AHA 2026 Cholesterol Guidelines
As per the Global Burden of Disease Study 2021, the burden of heart failure in adolescents and young adults aged 10–24 years is increasing globally.
The guidelines call for early intervention through early screening and healthy lifestyle changes, starting from childhood.
It recommends:
- Children (9-11 years): Cholesterol screening if never done before.
- Adults (30-79 years): Evaluate 10- and 30-year ASCVD risk to determine the need for early intervention
- Considering lipid-lowering therapy for young adults with -- persistent LDL of at least 160 mg/dL, strong family history of ASCVD, and/or at least 10 percent 30-year risk for ASCVD
"They encourage us to think beyond the usual 5- or 10-year risk window and consider the long-term picture—what might happen 20 or 30 years down the road for someone in their 40s or 50s,” Dr. Johnson told HealthandMe.
Also read: ACC/AHA Cholesterol Guidelines 2026 Explained: Start Screening For Cardiovascular Diseases Early
Heart Disease: A Long-term Treatment
The heart expert also stated that chronic conditions like heart disease require long-term management—sometimes for decades—unlike an infection, where a two-week antibiotic course resolves the problem.
“One of the biggest challenges I see in clinics is that patients often come in after a dramatic event—chest pain, a heart attack, or a procedure. Alongside immediate treatment, I prescribe medications and recommend lifestyle changes. And then patients ask, ‘How long do I have to do this? This reflects a very different mindset”.
Dr. Johnson urged cardiologists and other healthcare workers to help patients understand, accept, and sustain these changes over the long term.
“Adjusting to the reality that life will be different for years or even a lifetime is not easy, but it’s essential,” he said.
Tuberculosis in 2026: Why It Still Remains India’s Silent Epidemic
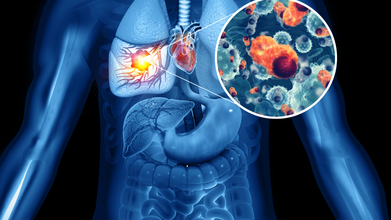
Credit: iStock
Step into a busy OPD, and you will see it: people coughing but not paying much attention. Tuberculosis is still around, just quietly spreading. By 2024, one out of every four global TB infections was recorded in India.
More than a number, each case hints at missed chances, tiny failures in spotting or stopping the disease that swell into widespread strain.
In earlier times, TB was common and very hard to recover from. Crowded homes, lack of fresh air, and low income open doors for germs to move fast. When hunger weakens people too, their bodies fail to hold back hidden sickness. But that is only part of what happens now. Conditions like smoking, drinking, high blood sugar, or HIV have slipped into view, tying daily habits closely to how often TB strikes.
After that, finding the right treatment can feel like a struggle. Some people start by visiting private clinics, shifting between different doctors until they finally learn what is wrong. Every wait means more time lost, moments when illness keeps growing without check.
Tuberculosis: What Takes The Biggest Toll?
Adults in their prime work phase feel it most. Males, particularly over the age of fifteen, carry heavier loads - a pattern the World Health Organization keeps pointing out. Yet biology alone doesn’t explain it.
Who shows up for treatment, who waits too long, who gets missed entirely, it's all written into the pattern. Older people, men, and anyone struggling with poor nutrition, using tobacco, or living with diabetes, show up more often in India’s national health data. The numbers tell a consistent story.
Tuberculosis: Late Symptoms
Here’s what happens. Tuberculosis usually shows up too late. Close to 60 percent of those feeling sick skip early help. Ongoing cough, body heat, weight loss, and night sweats are early signs. Some self-treat. For many, money becomes a barrier. Then comes the expected outcome - severe illness, tougher treatments, more time healing.
Still, false beliefs hang on. Air carries TB, not hands. Passing a meal does not pass the disease, yet shame can hold someone back from care. Cough that won’t quit, rising heat in the body, pounds slipping away, sweat at night - these hints show up early but get ignored till chances shrink.
Fighting TB in India isn’t only about medicine; it lives in habits, choices, and how people see illness. If getting help fast stays rare instead of routine, the disease keeps moving quietly through packed houses, buzzing health rooms.
Dr. Harish Bhatia is Senior Consultant in Pulmonary Medicine at Yatharth Hospital, New Delhi.
How Leg Stiffness Impacts Spine Health: Tips For Gen Z Fitness Enthusiasts

Credit: iStock
Today, the fitness scene has gained much traction among the Gen Z population. With more and more young people spending time in the gym and working out, it is important for fitness enthusiasts to remember the importance of leg stiffness and its impact on spine health. Leg stiffness has the potential to cause unnecessary strain on the spine and back during workouts.
From a neurosurgical point of view, we see that the spine is not just a mechanical support structure but a sensitive pathway through which the spinal cord and nerve roots run. Repeated micro-strain caused by poor flexibility can cause young patients to suffer early degenerative changes that may cause nerve irritation.
We also see that strengthening the abdominal muscles is essential in stabilizing the spine, thereby preventing disc injuries. Early intervention in minor complaints, such as back stiffness or nerve pain, is essential in preventing more serious problems that may need surgical intervention.
The Link Between Leg Stiffness And Spine Health
The muscles in your legs are important for your spine's health. The hamstring, hip flexor, and calf muscles are all significant players in the movement and positioning of your spine. Leg stiffness has the potential to cause unnecessary strain on the spine and back. Leg stiffness limits the movement and positioning of the hips and the spine.
When these muscle groups are tight, they alter pelvic alignment and increase load on the lumbar spine. Over time, this abnormal biomechanics can lead to disc stress and facet joint overload.
In neurosurgical practice, we often see young patients presenting with early symptoms of nerve compression where underlying muscle imbalance and stiffness play a contributory role.
Common Gym Mistakes That Increase The Risk
For young people, the main focus in the gym is on strength training, while flexibility and rest are ignored. This makes the condition of the legs stiffer. Another common error is improper posture while performing certain exercises in the gym. When the legs and hips are inflexible, proper posture is difficult, which causes pressure on the spine.
Sitting for a long time, studying, playing games on gadgets, etc., causes the hip flexors and the hamstring muscles in the legs to become stiffer, which causes pressure on the spine.
From a clinical standpoint, improper lifting techniques combined with stiffness can increase the risk of lumbar disc prolapse and nerve root irritation, conditions frequently encountered in spine clinics.
Tips to Prevent Spine Problems In The Gym
- Warm-ups: It is important to warm up the body before performing weightlifting exercises in the gym. It is recommended that the warm-up process take at least 5–10 minutes.
- Flexibility: It is important to include flexibility exercises in the gym routine, as they help in the proper movement of the legs, which in turn helps in preventing spine problems.
- Proper Posture: It is important to maintain proper posture while performing certain exercises in the gym, like squats, deadlifts, etc.
- Stretching After Workouts: This will help in the release of tension in the muscles and prevent the buildup of stiffness.
- Balance of Training and Recovery: This will help in maintaining the flexibility of the muscles and the spine.
Additionally, from a neurosurgical perspective, core strengthening plays a crucial role in stabilizing the spine and reducing the risk of disc-related injuries. Early attention to minor symptoms like back stiffness or radiating pain can prevent progression to more serious conditions requiring intervention.
Common Spine Problems To Avoid
Common spine problems to avoid during gym workouts include Herniated Disc, Sciatica, Spondylolisthesis, and Muscle Strain. These can occur from poor form, heavy lifting, or lack of warm-up.
In advanced cases, such conditions may lead to nerve compression requiring specialized evaluation and, rarely, surgical management. However, most of these issues are preventable with correct technique and conditioning.
Fitness enthusiasts in the Gen Z generation need to understand that it is very important to develop strength in the body while at the same time maintaining flexibility. The solution to the problem of a stiff leg is the foundation of protecting the spine and improving workout performance. This is achievable through the right warm-up, correct workout, and correct lifting.
Dr. Gaurav Batra is a Consultant - Neurosurgeon (Brain & Spine) at Max Hospital, Vaishali.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited