- Health Conditions A-Z
- Health & Wellness
- Nutrition
- Fitness
- Health News
- Ayurveda
- Videos
- Medicine A-Z
- Parenting
Study Shows Ebola Virus May Persist In Breast Milk For Over 3 Months After Recovery
Credit: Canva
Even after recovery, the deadly Ebola virus (EBOV) can persist for a longer duration — more than three months — in breastmilk, according to a case report.
Ebola virus disease (EVD) is a severe viral illness that has a 25 percent – 90 percent fatality rate.
Ebola in pregnancy raises significant complications ranging from spontaneous abortion to maternal and neonatal death.
In a case report published in the New England Journal of Medicine, a team of researchers from the Republic of Congo and Senegal shared the case history of a 23-year-old woman in whom Ebola was still detectable in breast milk at 14 weeks.
The case reported the rare occurrence of a pregnant woman who survived EVD with no complications, neither to the mother nor the baby. However, the deadly virus was still present in the mothers' breast milk, which cited the potential risk of post-illness transmission to infants.
What Is Ebola Virus Disease?
As per the World Health Organization (WHO), EVD is a rare but severe illness in humans and is often fatal.
People can get infected with the virus if they touch an infected animal when preparing food, or touch body fluids of an infected person such as saliva, urine, feces or semen, or things that have body fluids of an infected person like clothes or sheets.
Ebola enters the body through cuts in the skin or when one is touching their eyes, nose or mouth. Early symptoms include fever, fatigue and headache.
What Was The Case
The woman from the Democratic Republic of the Congo (DRC) contracted EBOV during pregnancy in 2019.
Soon after, she was administered monoclonal antibody therapy and was discharged after three negative reverse-transcriptase–polymerase-chain-reaction blood tests for EBOV.
The woman delivered a healthy baby at 42 weeks of gestation. No evidence of EBOV infection was found in maternal blood, amniotic fluid, vaginal secretions, or the newborn.
Ebola Detectable In Breast Milk At 14 Weeks
Yet surprisingly, the EBOV virus persisted in the placenta and breast milk.
Tests revealed that while the mother’s blood remained negative, viral RNA was still detectable in breast milk at 14 weeks after illness onset. To protect the newborn from transmission, clinicians used the drug bromocriptine to suppress lactation.
As per the World Health Organization (WHO) guidelines, the mother was also isolated from the baby and not breastfed. A prophylactic (preventive) monoclonal antibody was also given to the newborn. During follow-up, the infant exhibited no signs of infection.
Ebola Virus: WHO Guidelines
During the 2018–2020 EVD outbreak in the northeast of DRC, 3,481 confirmed cases were reported. Of these, nearly 60 percent occurred in females, and about 45 percent occurred in children below 18 years of age.
Current WHO guidance recommends that Ebola survivors avoid breastfeeding until viral clearance is confirmed.
The global health body advises women with suspected or confirmed Ebola to immediately stop breastfeeding and be prioritized for diagnostic testing.
Children exposed to Ebola through breast milk
- Must be placed under care,
- Closely monitored for symptoms over 21 days
- Fed with an appropriate breast milk substitute.
- Restarted on breastfeeding after two consecutive negative tests of breast milk.
Ebola Scare In India: Chhattisgarh Reports 3 Suspected Cases
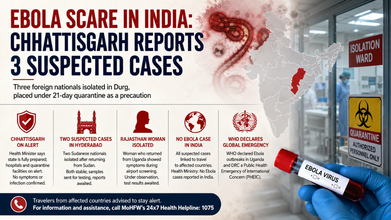
Credit: AI generated image
After Rajasthan and Hyderabad, Chhattisgarh today reported three suspected cases of Ebola involving foreign nationals.
According to media reports, the three have been isolated in Durg and placed under a 21-day quarantine as a precaution.
Chhattisgarh Health Minister Shyam Bihari Jaiswal announced that the state is fully prepared to handle any potential Ebola virus infection, stressing that hospitals and quarantine facilities have been put on alert and necessary arrangements are in place to ensure public safety.
Speaking to reporters, Jaiswal said the three individuals under observation were nationals from African countries and were being monitored in line with health protocols.
He added that no Ebola infection had been confirmed so far and that none of the individuals were showing symptoms of the disease.
"We have been fully prepared across the state at every level for a month now. The three individuals placed in isolation in Durg are nationals from African countries and have been quarantined for 21 days as a precautionary measure. So far, tests have not confirmed the presence of the virus, nor are they exhibiting any symptoms," he said.
Two Suspected Cases In Hyderabad
Earlier, two people in Hyderabad who returned from Sudan were isolated.
A Sudanese national, a student in his 20s, with a fever, was admitted to the state-run Gandhi Hospital. The student's condition improved, and he had no fever on Friday morning. His attendant was advised to stay in isolation at home, according to media reports.
Also read: WHO Says Ebola Fight Is Catching Up; Expert Explains Science Behind Patient Recoveries
Another Sudanese national, who arrived at Rajiv Gandhi International Airport a day earlier, was also shifted to the isolation ward of Gandhi Hospital for further tests after he was found to have a fever during thermal screening at the airport. The 35-year-old, who had come to Hyderabad for knee surgery, had no fever as of Friday morning and was asymptomatic, officials said.
Samples containing oral and nasal swabs have been collected and will be sent to the Centre for Cellular and Molecular Biology (CCMB) for testing. Test reports of both individuals are awaited.
Rajasthan Woman Isolated
Meanwhile, Rajasthan has also isolated one woman who returned from Uganda following symptoms.
During routine health screening at the airport, she exhibited symptoms associated with Ebola infection. The health department was immediately informed, and she was placed under special observation.
While she has displayed symptoms similar to Ebola infection, confirmation can only be made after laboratory testing. The results are awaited.
No Ebola Case Reported In India
Read More: Bundibugyo Ebola Outbreak: WHO Identifies Experimental Treatments, Vaccines
All suspected cases have been linked to travel to Ebola-affected countries such as Uganda, the Democratic Republic of Congo, and Sudan.
"No Ebola disease cases have been reported in India," the Health Ministry said in its latest update on June 3. The Health Ministry has also advised travelers arriving from Ebola-affected countries, including Uganda and the Democratic Republic of Congo, to remain alert for symptoms and seek medical guidance if they feel unwell.
"For information, guidance, and assistance, call MoHFW's 24x7 Health Helpline: 1075," the ministry said on X.
Ebola: A Global Health Emergency
On May 17, the World Health Organization classified the Ebola outbreaks in Uganda and the Democratic Republic of Congo as a Public Health Emergency of International Concern (PHEIC).
A total of 452 Ebola cases have been confirmed in the Democratic Republic of Congo, including 82 deaths. Uganda has reported 16 confirmed cases.
Meanwhile, the number of suspected cases has fallen from more than 1,000 last week to 116 as health teams work through the backlog. Six people in the DRC and two in Uganda have recovered to date.
WHO Says Ebola Fight Is Catching Up; Expert Explains Science Behind Patient Recoveries

Credit: Canva/WHO
After previously warning that Ebola was "outpacing us," WHO Director-General Tedros Adhanom Ghebreyesus said on Thursday that "we are catching up" as efforts to contain the outbreak in the Democratic Republic of Congo show progress.
A total of 452 Ebola cases have been confirmed in the Democratic Republic of Congo, including 82 deaths. Uganda has reported 16 confirmed cases. Meanwhile, the number of suspected cases has fallen from more than 1,000 last week to 116 as health teams work through the backlog.
WHO Sees Signs of Progress
“What I saw gave me hope,” Ghebreyesus said at a press conference.
“The outbreak had a big head start, and we're still behind, but under the leadership of the Government of DRC, we are catching up,” he added.
Importantly, he noted that six people in the DRC and two in Uganda have recovered to date, “showing that people can survive Ebola if they have access to care and go to health facilities as soon as they show symptoms.”
Why Are Patients Recovering?
The latest outbreak is caused by the Bundibugyo strain of the Ebola virus, for which there is currently neither a vaccine nor an antiviral treatment. So how are patients recovering?
Dr. Rajeev Jayadevan, Co-Chairman of the National IMA COVID Task Force and Past President of the Indian Medical Association, Cochin, told HealthandMe that a combination of factors—including the virus strain, access to medical care, and individual immune responses—can significantly influence whether a patient survives the disease.

Ebola virus disease is a severe illness caused by different strains of the Ebola virus. The current outbreak is linked to the Bundibugyo strain, which has a lower mortality rate than the more lethal Zaire strain responsible for several previous outbreaks, he said.
“The mortality of Ebola virus disease is tied to several components,” Dr. Rajeev explained.
Early Medical Care Improves Survival
One of the most important factors is access to early medical attention and supportive care. Patients who receive prompt treatment at well-equipped healthcare facilities staffed by experienced healthcare workers have a much greater chance of survival.
However, such healthcare access is often limited in outbreak-affected regions of Africa due to ongoing conflicts and socioeconomic challenges.
“The chance of survival is much higher if a person receives good medical attention and early supportive care,” he said.
Bundibugyo Strain vs Zaire Strain
Also read: Ebola Bundibugyo Strain: All You Should Know About The Rare Virus
The strain of the virus also plays a critical role. Dr. Rajeev said that because the Bundibugyo strain is less lethal than the Zaire strain, more infected individuals are expected to survive under similar conditions.
“If a hundred people get infected with the Zaire strain and another hundred with the Bundibugyo strain, more people in the Bundibugyo group will survive, all other conditions remaining the same,” he said.
Difference In Immune Response
Another important factor is the body's immune response, which varies from person to person. Dr. Rajeev highlighted the role of human leukocyte antigens (HLA), proteins that help the immune system recognize and respond to invading pathogens. Because each individual's HLA profile is unique, people infected with the same virus can generate different immune responses.
“HLA works closely with the immune system by presenting pieces of the virus to immune cells, helping the body build a targeted response,” he said.
Also read: Ebola Alert In India: Rajasthan, Hyderabad Report Suspected Cases of Deadly Virus
This biological diversity is one reason why the same infection can affect individuals differently. It is also considered an evolutionary safeguard that helps prevent a single pathogen from devastating the entire human population.
The Role of Probability
Dr. Rajeev also pointed to a simple statistical reality. “If the mortality rate in the current outbreak is around 30 per cent, that means about 70 per cent of infected individuals are expected to survive,” he said.
According to the expert, survival often results from a combination of favorable factors, including infection with a less lethal strain, timely medical care, a strong immune response, and the overall probability of recovery within a given outbreak.
Ovarian Cancer: UK NHS Rolls Out First Major Drug In Over 20 Years

Credit: Canva
The UK National Health Service (NHS) has approved the free rollout of a breakthrough ovarian cancer drug, benefiting hundreds of women with hard-to-treat cancer starting today.
Importantly, the US FDA-approved drug is the first new addition to NHS treatment for this group of patients in over 20 years.
The last major NHS treatment introduced for these patients was the rollout of liposomal doxorubicin and paclitaxel in the early 2000s.
The NHS, in a statement, said that the new targeted therapy, mirvetuximab soravtansine, will be offered to patients living with ovarian cancer whose disease has stopped responding to standard (platinum-based) chemotherapy, providing new hope of extra time to live.
Mirvetuximab soravtansine (Elahere) has been developed by AbbVie. The NHS estimates up to 400 patients in England each year could benefit.
“This represents the most significant breakthrough in NHS treatment for these hard-to-treat ovarian cancers in over two decades – and we’re delighted it will now offer hundreds of women much-needed hope of precious extra time with their loved ones,” said Professor Ruth Plummer, NHS national clinical lead for cancer drugs.
How Does The Drug Work?
According to the NHS, the drug combines a ‘homing’ antibody with a cancer-killing medicine, often described by scientists as a ‘biological missile’ or ‘Trojan horse’ therapy.
It works by attaching to ovarian cancer cells that have a protein called folate receptor alpha (FRα) on their surface, before releasing a cancer-killing molecule that destroys the cell from within.
In a major global clinical trial involving eight NHS hospitals, the treatment delayed cancer progression and prolonged survival, with patients living 16.5 months on average compared to 12.8 months with chemotherapy.
Also read: New Pancreatic Cancer Drug Daxaronrasib May Benefit Patients With Lung And Ovarian Tumors Too
Who Can Avail The Drug Through The NHS?
Following a recommendation by the National Institute for Health and Care Excellence (NICE), the treatment will be available for:
- patients with epithelial ovarian cancer,
- peritoneal or fallopian tube cancer that has become resistant to platinum-based chemotherapy
- whose tumors contain the FRα protein targeted by the drug.
The treatment is given intravenously (via a drip) over two to four hours, once every three weeks.
Are There Any Side Effects?
The NHS stated that the drug may also have more tolerable side effects than traditional chemotherapy, as it is aimed more precisely at cancer cells than chemotherapy, which can also harm healthy cells.
Common side effects include:
- Eye problems such as blurred vision or dry eyes
- Tiredness
- Nausea
- Low blood counts
Most side effects are manageable with monitoring and supportive care.
Read More: Alan Brazil Shares Survival Story After Heart Stopped During Liver Transplant
Ovarian Cancer Remains A Major Health Challenge
Ovarian cancer is one of the leading causes of death from gynecological cancer worldwide. In the UK, there are around 7,500 new diagnoses each year.
Standard treatment for ovarian cancer typically involves surgery and chemotherapy, but around 80 per cent of patients with advanced disease relapse, and most eventually develop resistance to chemotherapy.
More than a third of patients (37 per cent) treated with mirvetuximab soravtansine also saw their tumors shrink by at least 30 per cent, compared to 16 per cent of patients receiving chemotherapy in clinical trials.
- Follow Us :



© 2024 Bennett, Coleman & Company Limited